Ntekim Atara, Campbell Oladapo, Rothenbacher Dietrich
College of Medicine, University of Ibadan, Ibadan, Nigeria.
Institute of Epidemiology and Medical Biometry, Ulm University, Ulm, Germany.
Cancer Med. 2015 Sep;4(9):1381-93. doi: 10.1002/cam4.485. Epub 2015 Jul 1.
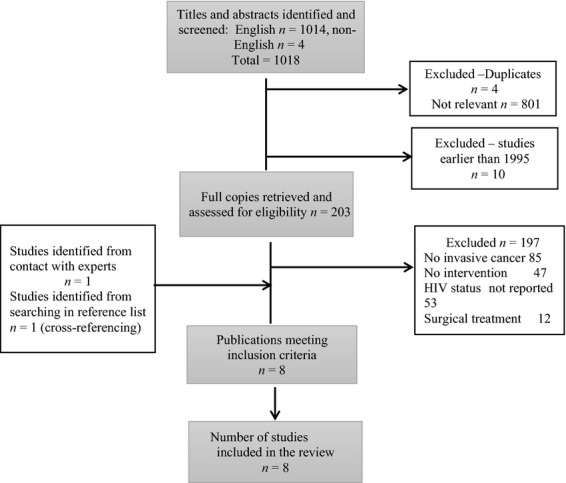
The clinical management of cervical cancer in HIV-positive patients has challenges mainly due to the concerns on immune status. At present, their mode of management is similar to HIV-seronegative patients involving the use of chemotherapy and radiotherapy concurrently as indicated. HIV infection, cancer, radiotherapy, and chemotherapy lower immunity through reduction in CD4 cell counts. At present there are no treatment guidelines for HIV-positive patients. This study was done to systematically review the literature on cervical cancer management in HIV-positive patients and treatment outcomes. A systematic literature search was done in the major databases to identify studies on the management of HIV-positive patients with cervical cancer. Identified studies were assessed for eligibility and inclusion in the review following the guidelines of The Cochrane Handbook for Systematic Reviews and CRD's (Centre for Reviews and Dissemination) guidance for undertaking reviews in health care. Eight eligible studies were identified from the literature. Three of them were prospective while five were retrospective studies. Notably, the average age at diagnosis of cervical cancer in HIV-positive patients was a decade lower than in seronegative patients. There was no difference in distribution of stages of disease at presentation between HIV-positive and negative patients. Mild acute toxicity (Grades 1 and 2) was higher in HIV-positive patients than in HIV-negative patients in hematopoietic system. In the grades 3 and 4 reactions, anemia was reported in 4% versus 2% while gastrointestinal reactions were reported in 5% versus 2% respectively. In general, patients who were started early on HAART had higher rates of treatment completion. The study supports the suggestion that HAART should be commenced early at cervical cancer diagnosis in HIV-positive patients diagnosed with cervical cancer to ensure less toxicity and better treatment compliance.
HIV阳性患者宫颈癌的临床管理面临诸多挑战,主要是由于对免疫状态的担忧。目前,他们的管理模式与HIV血清阴性患者相似,即根据需要同时使用化疗和放疗。HIV感染、癌症、放疗和化疗会通过降低CD4细胞计数来降低免疫力。目前尚无针对HIV阳性患者的治疗指南。本研究旨在系统回顾关于HIV阳性患者宫颈癌管理及治疗结果的文献。在主要数据库中进行了系统的文献检索,以确定关于HIV阳性宫颈癌患者管理的研究。根据《Cochrane系统评价手册》的指南以及CRD(卫生保健系统评价中心)进行系统评价的指导原则,对纳入的研究进行资格评估和纳入审查。从文献中确定了8项符合条件的研究。其中3项为前瞻性研究,5项为回顾性研究。值得注意的是,HIV阳性患者宫颈癌诊断时的平均年龄比血清阴性患者低十年。HIV阳性和阴性患者就诊时疾病分期的分布没有差异。HIV阳性患者造血系统的轻度急性毒性(1级和2级)高于HIV阴性患者。在3级和4级反应中,贫血报告率分别为4%和2%,胃肠道反应报告率分别为5%和2%。一般来说,早期开始接受高效抗逆转录病毒治疗(HAART)的患者治疗完成率更高。该研究支持这样的建议,即对于诊断为宫颈癌的HIV阳性患者,应在宫颈癌诊断时尽早开始HAART,以确保毒性更小且治疗依从性更好。