Litwińska Ewelina, Nowak Marek, Kolasa-Zwierzchowska Dorota, Nowińska-Serwach Anna, Władziński Jacek, Szpakowski Artur, Szpakowski Marian, Wilczyński Jacek R
Perinatology and Gynecology Department, Polish Mother's Memorial Hospital-Research Institute, Łódź, Poland.
Gynecology and Gynecologic Oncology Department, Polish Mother's Memorial Hospital-Research Institute, Łódź, Poland.
Prz Menopauzalny. 2014 Sep;13(4):242-6. doi: 10.5114/pm.2014.45000. Epub 2014 Sep 9.
Uterine leiomyomas are the most common benign tumors of the female reproductive system. Although the majority of myomas are asymptomatic, some patients have symptoms or signs of varying degrees and require a hysterectomy.
The aim of the study was to compare the clinical results of two minimally invasive hysterectomy techniques: vaginal hysterectomy (VH) and laparoscopically assisted vaginal hysterectomy (LAVH).
A retrospective, observational study was performed at a tertiary care center: the Gynecology and Gynecologic Oncology Department, Polish Mother's Memorial Hospital Research Institute. The study period was from January 2003 to December 2012. A total of 159 women underwent either vaginal hysterectomy (VH, n = 120) or laparoscopically assisted vaginal hysterectomy (LAVH, n = 39) for symptomatic uterine myomas. Outcome measures, including past medical history, blood loss, major complications, operating time and discharge time were assessed and compared between the studied groups. Statistical analysis was performed using Student t-test, U-Mann Whitney test, χ(2) test and Yates'χ(2) test. P < 0.05 was considered statistically significant.
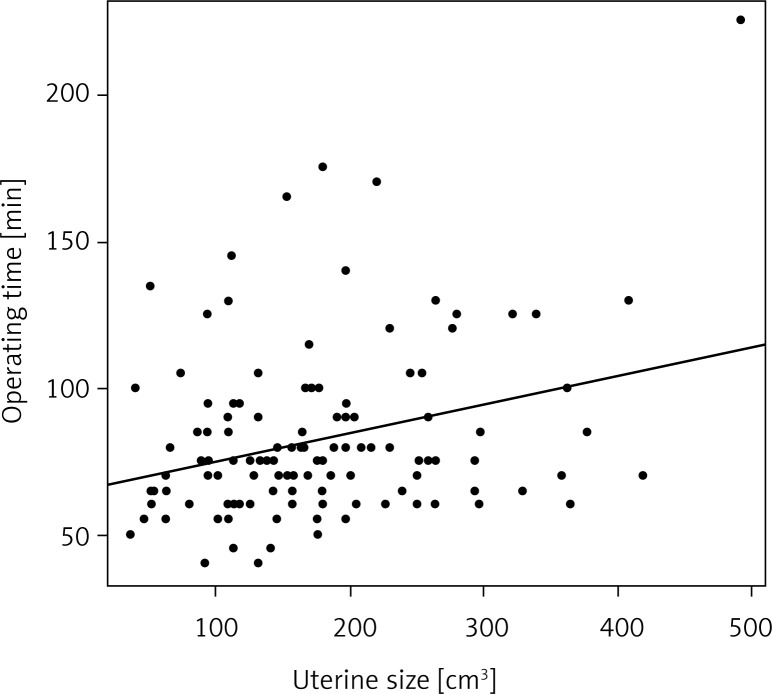
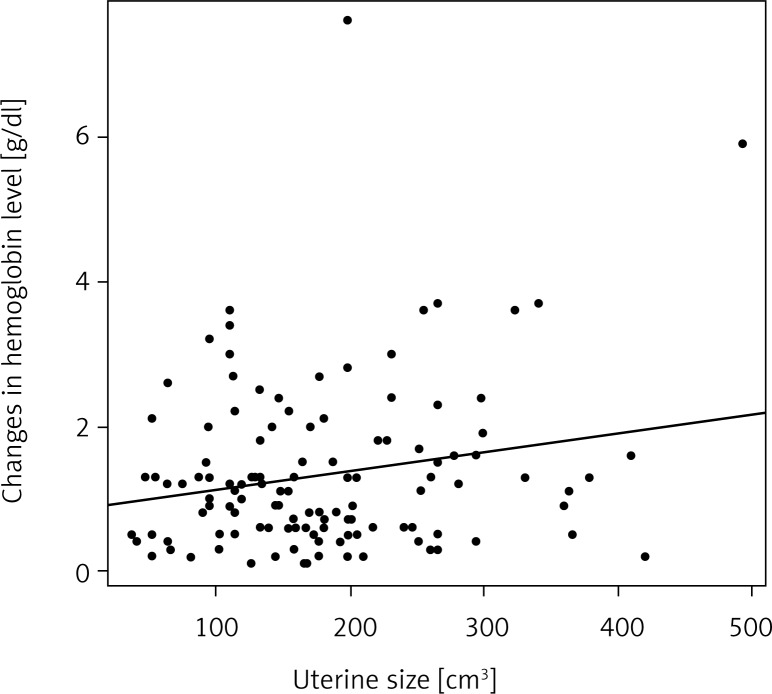
There were no differences in patients' mean age. Parity was significantly higher in the VH group (VH 1.9 ± 0.7 vs. LAVH 1.5 ± 0.8; p = 0.008). No difference was found in the mean ± standard deviation (SD) uterine volume between vaginal hysterectomy and LAVH groups (179 ± 89 vs. 199 ± 88 cm(3)), respectively. The mean operative time was significantly longer for the LAVH group (83 ± 29 vs. 131 ± 30 min; p = 0.0001). The intraoperative blood loss (VH 1.3 ± 1.1 vs. LAVH 1.4 ± 0.9 g/dl; p = 0.2) and the rate of intra- and postoperative complications were similar in both groups studied. The mean discharge time was longer for LAVH than for VH (VH 4.2 ± 1.2 vs. LAVH 5.3 ± 1.3 days, p = 0.0001).
Laparoscopically assisted vaginal hysterectomy and VH are safe hysterectomy techniques for women with the myomatous uterus. Concerning the LAVH, the abdominal-pelvic exploration and the ability to perform adnexectomy safely represent the major advantages comparing with VH. Vaginal hysterectomy had a shorter operating time and the mild blood loss making it a suitable method of hysterectomy for cases in which the shortest duration of surgery and anesthesia is preferable.
子宫平滑肌瘤是女性生殖系统最常见的良性肿瘤。尽管大多数肌瘤无症状,但一些患者有不同程度的症状或体征,需要进行子宫切除术。
本研究的目的是比较两种微创子宫切除术技术的临床结果:阴道子宫切除术(VH)和腹腔镜辅助阴道子宫切除术(LAVH)。
在一家三级医疗中心——波兰母亲纪念医院研究所妇产科和妇科肿瘤学部进行了一项回顾性观察研究。研究期间为2003年1月至2012年12月。共有159名女性因有症状的子宫肌瘤接受了阴道子宫切除术(VH,n = 120)或腹腔镜辅助阴道子宫切除术(LAVH,n = 39)。评估并比较了研究组之间的结果指标,包括既往病史、失血量、主要并发症、手术时间和出院时间。使用学生t检验、U-曼-惠特尼检验、χ²检验和耶茨χ²检验进行统计分析。P < 0.05被认为具有统计学意义。
患者的平均年龄无差异。VH组的产次显著更高(VH 1.9 ± 0.7 vs. LAVH 1.5 ± 0.8;p = 0.008)。阴道子宫切除术组和LAVH组之间的平均子宫体积(标准差)(SD)无差异(分别为179 ± 89 vs. 199 ± 88 cm³)。LAVH组的平均手术时间显著更长(83 ± 29 vs. 131 ± 30分钟;p = 0.0001)。两组的术中失血量(VH 1.3 ± 1.1 vs. LAVH 1.4 ± 0.9 g/dl;p = 0.2)以及术中和术后并发症发生率相似。LAVH组的平均出院时间比VH组长(VH 4.2 ± 1.2 vs. LAVH 5.3 ± 1.3天,p = 0.0001)。
腹腔镜辅助阴道子宫切除术和VH对于患有肌瘤性子宫的女性来说是安全的子宫切除技术。关于LAVH,与VH相比,腹盆腔探查以及安全进行附件切除术的能力是主要优势。阴道子宫切除术的手术时间较短且失血量少,使其成为手术和麻醉时间最短为首选情况的合适子宫切除方法。