Manto Mario, Mariën Peter
Unité d'Etude du Mouvement, FNRS-ULB Erasme, 808 Route de Lennik, 1070 Bruxelles, Belgium.
Clinical and Experimental Neurolinguistics, Vrije Universiteit Brussel, Pleinlaan 2, 1050 Brussels, Belgium ; Department of Neurology and Memory Clinic, ZNA General Hospital Middelheim, Lindendreef 1, 2020 Antwerp, Belgium.
Cerebellum Ataxias. 2015 Feb 27;2:2. doi: 10.1186/s40673-015-0023-1. eCollection 2015.
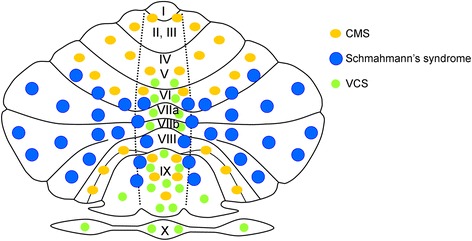
Schmahmann's syndrome represents a novel clinical condition consisting of a constellation of cognitive and affective deficits following cerebellar disease. The complex was first described in 1998 as cerebellar cognitive affective syndrome (CCAS) on the basis of a careful neurological examination, detailed bedside mental state tests, neuropsychological investigations and anatomical neuroimaging of a group of 20 patients with focal cerebellar disorders. The syndrome was characterized by four clusters of symptoms including: (a) impairment of executive functions such as planning, set-shifting, verbal fluency, abstract reasoning and working memory, (b) impaired visuo-spatial cognition, (c) personality changes with blunting of affect or abnormal behaviour, and (d) language deficits including agrammatism, wordfinding disturbances, disruption of language dynamics and dysprosodia. This complex of neurocognitive and behavioural-affective symptoms was ascribed to a functional disruption of the reciprocal pathways that connect the cerebellum with the limbic circuitry and the prefrontal, temporal and parietal association cortices. With the introduction of Schmahmann's syndrome, clinical ataxiology has found its third cornerstone, the two others being the cerebellar motor syndrome (CMS) mainly delineated by the pioneer French and English neurologists of the 19(th) and early 20(th) century, and the vestibulo-cerebellar syndrome (VCS) consisting of ocular instability, deficits of oculomotor movements and ocular misalignment.
施马曼综合征是一种新的临床病症,由小脑疾病后出现的一系列认知和情感缺陷组成。1998年,在对一组20例局灶性小脑疾病患者进行仔细的神经学检查、详细的床边精神状态测试、神经心理学调查和解剖神经成像的基础上,该综合征首次被描述为小脑认知情感综合征(CCAS)。该综合征的特征包括四组症状:(a)执行功能受损,如计划、转换任务、言语流畅性、抽象推理和工作记忆;(b)视觉空间认知受损;(c)人格改变,情感迟钝或行为异常;(d)语言缺陷,包括语法缺失、找词困难、语言动态障碍和韵律障碍。这种神经认知和行为情感症状的复合体被归因于连接小脑与边缘系统以及前额叶、颞叶和顶叶联合皮质的交互通路的功能破坏。随着施马曼综合征的提出,临床共济失调学找到了其第三个基石,另外两个基石是主要由19世纪和20世纪初的法国和英国神经学先驱所描述的小脑运动综合征(CMS),以及由眼球不稳定、眼球运动缺陷和眼球错位组成的前庭小脑综合征(VCS)。