Harada Taisuke, Abe Takashige, Kato Fumi, Matsumoto Ryuji, Fujita Hiromi, Murai Sachiyo, Miyajima Naoto, Tsuchiya Kunihiko, Maruyama Satoru, Kudo Kohsuke, Shinohara Nobuo
Department of Diagnostic and Interventional Radiology, Hokkaido University Hospital, Sapporo, Japan.
Department of Urology, Hokkaido University Graduate School of Medicine, North-15, West-7, North Ward, Sapporo, 060-8638, Japan.
BMC Urol. 2015 Sep 4;15:91. doi: 10.1186/s12894-015-0087-5.
To clarify the relationship between the probability of prostate cancer scaled using a 5-point Likert system and the biological characteristics of corresponding tumor foci.
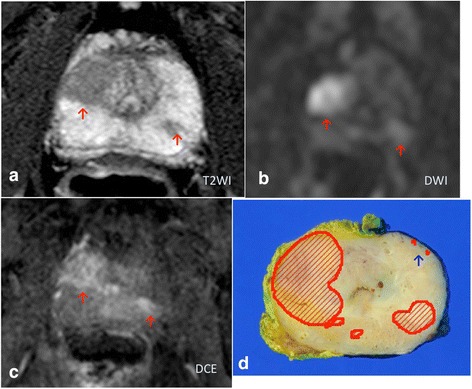
The present study involved 44 patients undergoing 3.0-Tesla multiparametric MRI before laparoscopic radical prostatectomy. Tracing based on pathological and MRI findings was performed. The relationship between the probability of cancer scaled using the 5-point Likert system and the biological characteristics of corresponding tumor foci was evaluated.
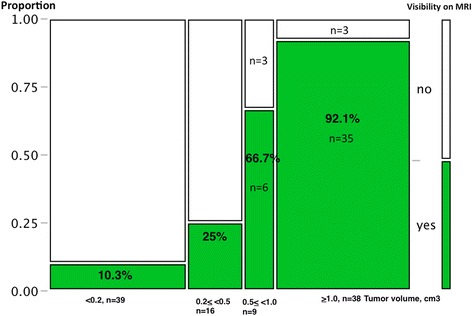
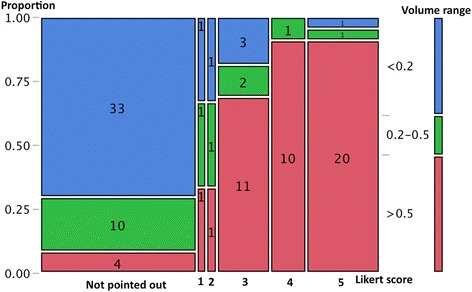
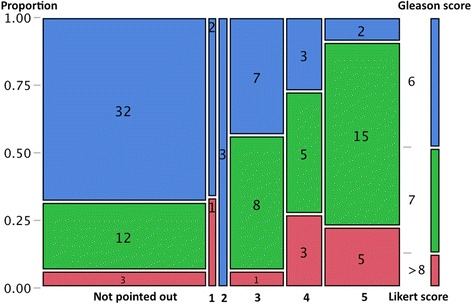
A total of 102 tumor foci were identified histologically from the 44 specimens. Of the 102 tumors, 55 were assigned a score based on MRI findings (score 1: n = 3; score 2: n = 3; score 3: n = 16; score 4: n = 11 score 5: n = 22), while 47 were not pointed out on MRI. The tracing study revealed that the proportion of >0.5 cm(3) tumors increased according to the upgrade of Likert scores (score 1 or 2: 33%; score 3: 68.8%; score 4 or 5: 90.9%, χ(2) test, p < 0.0001). The proportion with a Gleason score >7 also increased from scale 2 to scale 5 (scale 2: 0%; scale 3: 56.3%; scale 4: 72.7%; 5: 90.9%, χ(2) test, p = 0.0001). On using score 3 or higher as the threshold of cancer detection on MRI, the detection rate markedly improved if the tumor volume exceeded 0.5 cm(3) (<0.2 cm(3): 10.3%; 0.2-0.5 cm(3): 25%; 0.5-1.0 cm(3): 66.7%; 1.0 < cm(3): 92.1%).
Each Likert scale favobably reflected the corresponding tumor's volume and Gleason score. Our observations show that "score 3 or higher" could be a useful threshold to predict clinically significant carcinoma when considering treatment options.
明确采用5分制李克特量表对前列腺癌可能性进行评分与相应肿瘤病灶生物学特征之间的关系。
本研究纳入44例在腹腔镜前列腺癌根治术前接受3.0T多参数磁共振成像(MRI)检查的患者。基于病理和MRI检查结果进行追踪。评估采用5分制李克特量表对癌症可能性进行评分与相应肿瘤病灶生物学特征之间的关系。
从44份标本中组织学鉴定出共102个肿瘤病灶。在这102个肿瘤中,55个根据MRI检查结果进行了评分(评分1:n = 3;评分2:n = 3;评分3:n = 16;评分4:n = 11;评分5:n = 22),而47个在MRI上未被指出。追踪研究显示,大于0.5cm³的肿瘤比例随李克特评分的升高而增加(评分1或2:33%;评分3:68.8%;评分4或5:90.9%,χ²检验,p < 0.0001)。Gleason评分>7的比例也从量表2到量表5逐渐增加(量表2:0%;量表3:56.3%;量表4:72.7%;量表5:90.9%,χ²检验,p = 0.0001)。以评分3及以上作为MRI上癌症检测的阈值,当肿瘤体积超过0.5cm³时,检测率显著提高(<0.2cm³:10.3%;0.2 - 0.5cm³:25%;0.5 - 1.0cm³:66.7%;1.0 < cm³:92.1%)。
每个李克特量表都能较好地反映相应肿瘤的体积和Gleason评分。我们的观察结果表明,在考虑治疗方案时,“评分3及以上”可能是预测临床显著癌的有用阈值。