Lovegrove Catherine Elizabeth, Matanhelia Mudit, Randeva Jagpal, Eldred-Evans David, Tam Henry, Miah Saiful, Winkler Mathias, Ahmed Hashim U, Shah Taimur T
Division of Surgery, Department of Surgery and Cancer, Imperial College London, London, UK.
Imperial Urology, Charing Cross Hospital, Imperial College Healthcare NHS Trust, London, UK.
Transl Androl Urol. 2018 Sep;7(Suppl 4):S420-S435. doi: 10.21037/tau.2018.07.06.
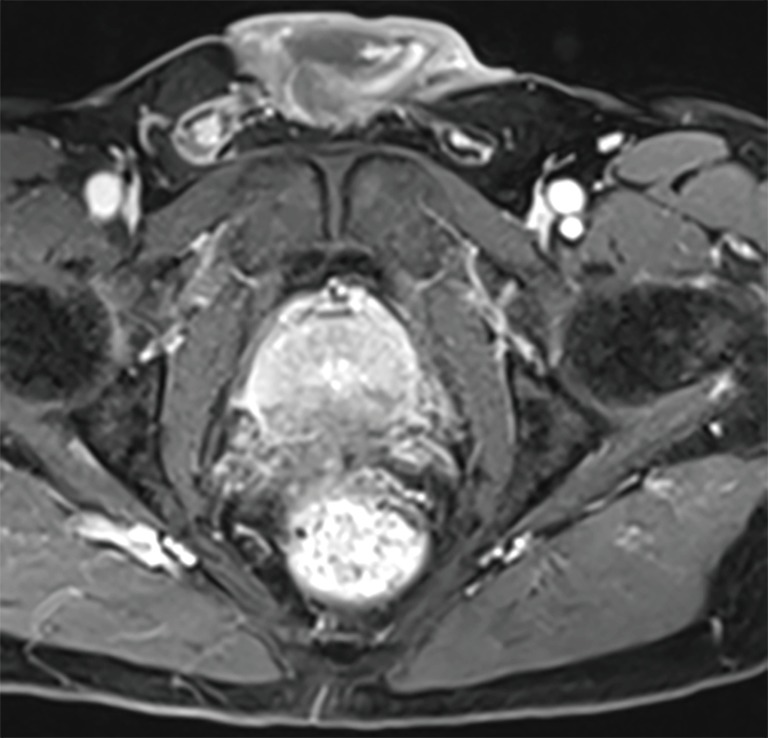
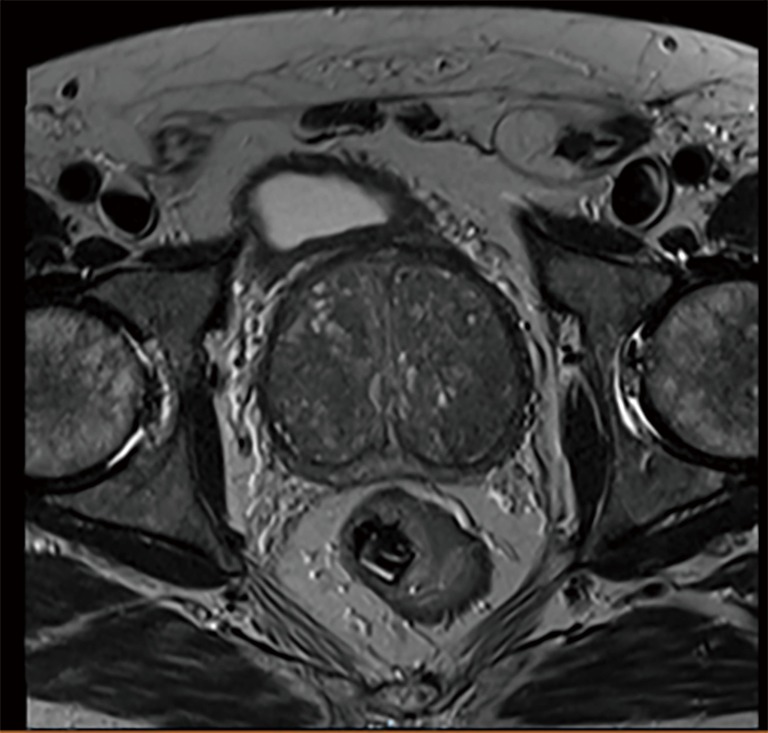
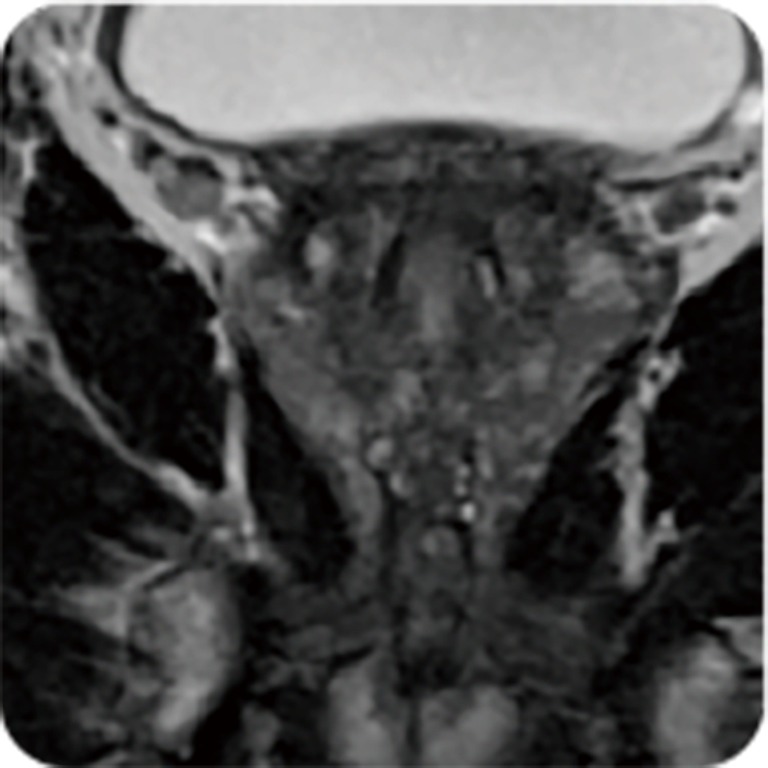
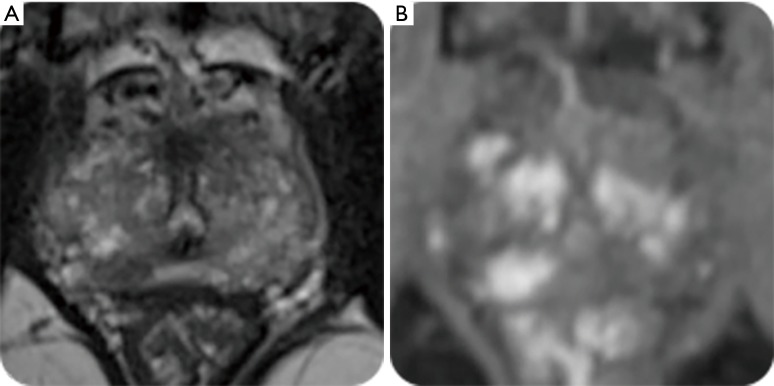
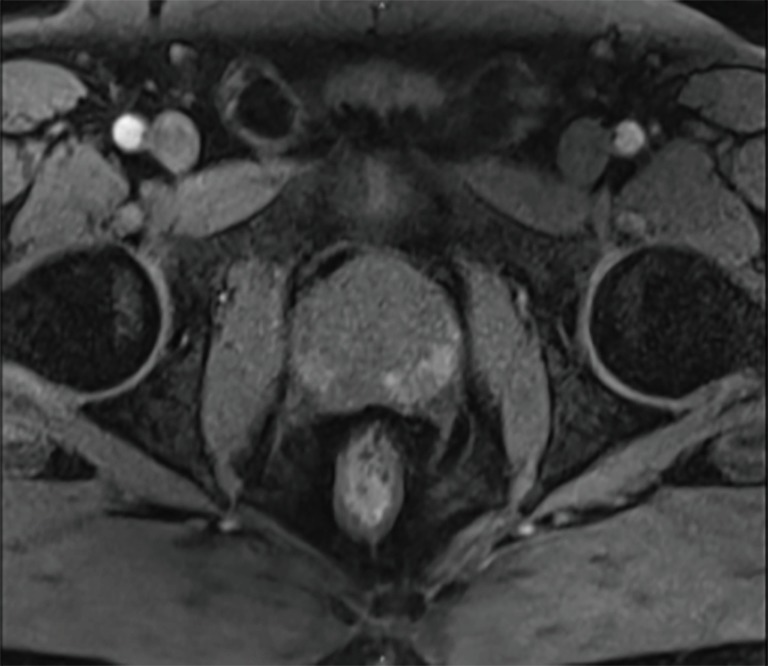
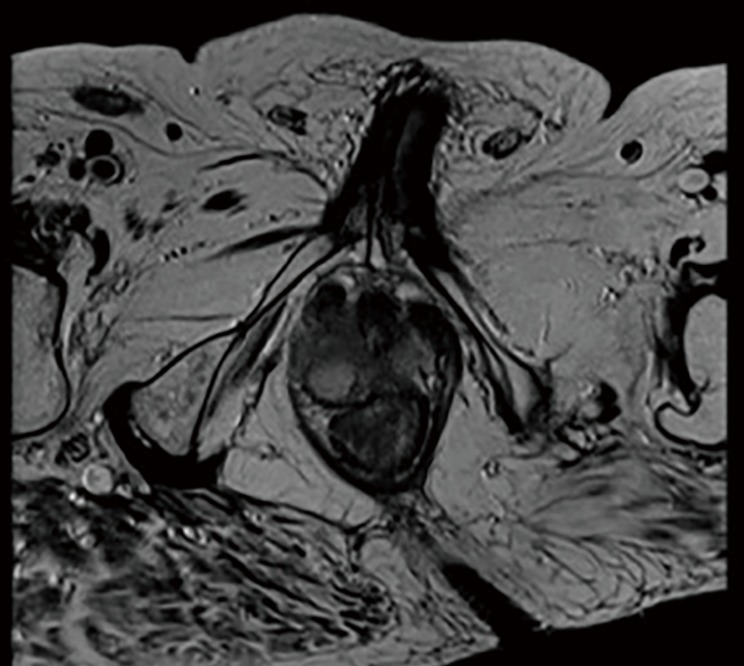
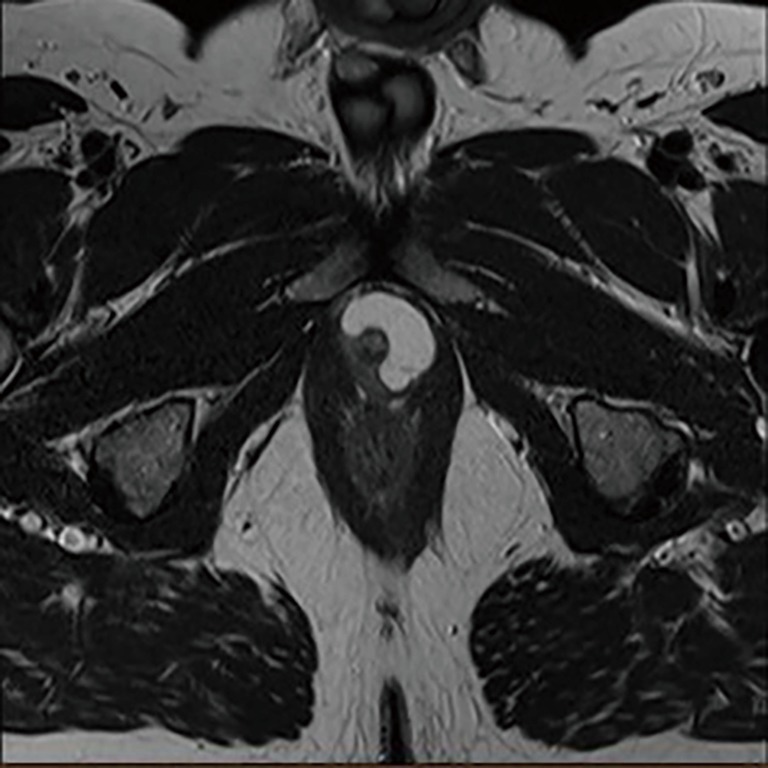
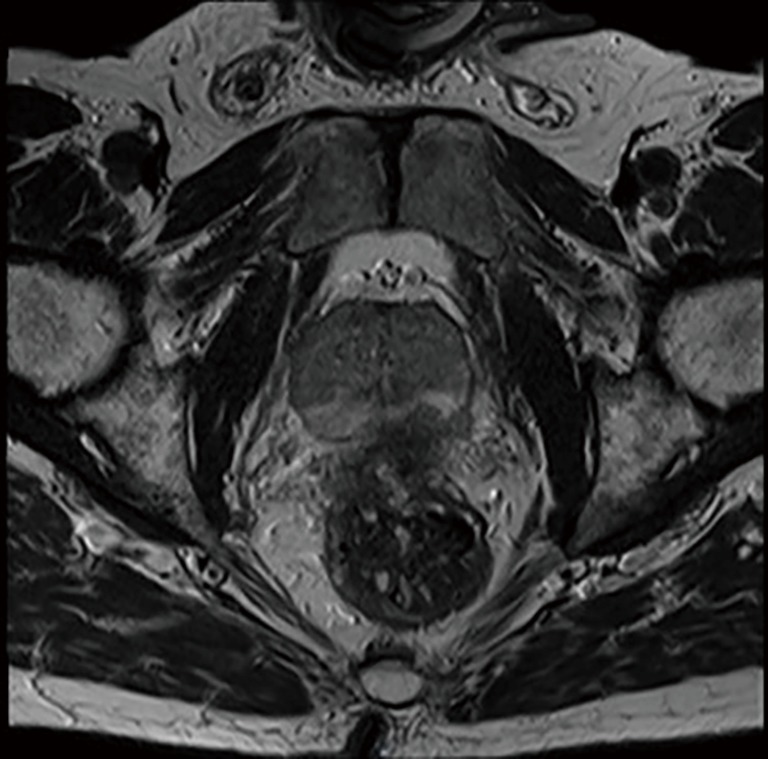
Accurate diagnosis of clinically significant prostate cancer is essential in identifying patients who should be offered treatment with curative intent. Modifications to the Gleason grading system in recent years show that accurate grading and reporting at needle biopsy can improve identification of clinically significant prostate cancers. Extracapsular extension of prostate cancer has been demonstrated to be an adverse prognostic factor with greater risk of metastatic spread than organ-confined disease. Tumor volume may be an independent prognostic factor and should be considered in conjunction with other factors. Multi-parametric magnetic resonance imaging (MP-MRI) has become an increasingly important tool in the diagnosis and characterization of prostate cancer. MP-MRI allows T2-weighted (T2W) anatomical imaging to be combined with functional and physiological assessment. Diffusion-weighted imaging (DWI) has shown greater sensitivity, specificity and negative predictive value compared to prostate specific antigen (PSA) testing and T2W imaging alone and has a more positive correlation with Gleason score and tumour volume. Dynamic gadolinium contrast-enhanced (DCE) imaging can exhibit difficulties in distinguishing prostatitis from malignancy in the peripheral zone, and between benign prostatic hyperplasia (BPH) and malignancies in the transition zone (TZ). Computer aided diagnosis utilizes software to aid radiologists in detecting and diagnosing abnormalities from diagnostic imaging. New techniques of quantitative MRI, such as VERDICT MRI use tissue-specific factors to delineate different cellular and microstructural phenotypes, characterizing tissue properties with greater detail. Proton MR spectroscopic imaging (MRSI) is a more technically challenging imaging modality than DCE and DWI MRI. Over the last decade, choline and prostate-specific membrane antigen (PSMA) positron emission tomography (PET) have developed as better tools for staging than conventional imaging. While hyperpolarized MRI shows promise in improving the imaging and differentiation of benign and malignant lesions there is further work required. Accurate reading and interpretation of diagnostic investigations is key to accurate identification of abnormal areas requiring biopsy, sparing those in whom benign or indolent disease can be managed by non-invasive means. Embracing and advancing existing technologies is essential in furthering this process.
准确诊断具有临床意义的前列腺癌对于确定适合进行根治性治疗的患者至关重要。近年来对 Gleason 分级系统的修改表明,在穿刺活检时进行准确分级和报告可改善对具有临床意义的前列腺癌的识别。前列腺癌的包膜外侵犯已被证明是一个不良预后因素,其转移扩散风险高于器官局限性疾病。肿瘤体积可能是一个独立的预后因素,应与其他因素结合考虑。多参数磁共振成像(MP-MRI)已成为前列腺癌诊断和特征描述中越来越重要的工具。MP-MRI 允许将 T2 加权(T2W)解剖成像与功能和生理评估相结合。与单独的前列腺特异性抗原(PSA)检测和 T2W 成像相比,扩散加权成像(DWI)显示出更高的敏感性、特异性和阴性预测价值,并且与 Gleason 评分和肿瘤体积具有更强的正相关性。动态钆对比增强(DCE)成像在区分外周区的前列腺炎与恶性肿瘤以及移行区(TZ)的良性前列腺增生(BPH)与恶性肿瘤方面可能存在困难。计算机辅助诊断利用软件帮助放射科医生从诊断成像中检测和诊断异常。定量 MRI 的新技术,如 VERDICT MRI,使用组织特异性因素来描绘不同的细胞和微观结构表型,更详细地表征组织特性。质子磁共振波谱成像(MRSI)是一种在技术上比 DCE 和 DWI MRI 更具挑战性的成像方式。在过去十年中,胆碱和前列腺特异性膜抗原(PSMA)正电子发射断层扫描(PET)已发展成为比传统成像更好的分期工具。虽然超极化 MRI 在改善良性和恶性病变的成像及鉴别方面显示出前景,但仍需要进一步开展工作。准确解读诊断检查对于准确识别需要活检的异常区域至关重要,使那些可通过非侵入性手段管理的良性或惰性疾病患者免受活检。采用和推进现有技术对于推进这一过程至关重要。