Kummer Benjamin R, Bhave Prashant D, Merkler Alexander E, Gialdini Gino, Okin Peter M, Kamel Hooman
Department of Neurology, Neurological Institute of New York, Columbia University College of Physicians and Surgeons, New York, NY (B.R.K.).
Division of Cardiology, University of Iowa Carver College of Medicine, Iowa City, IA (P.D.B.).
J Am Heart Assoc. 2015 Sep 22;4(9):e002097. doi: 10.1161/JAHA.115.002097.
Catheter ablation is increasingly used for rhythm control in symptomatic atrial fibrillation (AF), but the demographic characteristics of patients undergoing this procedure are unclear.
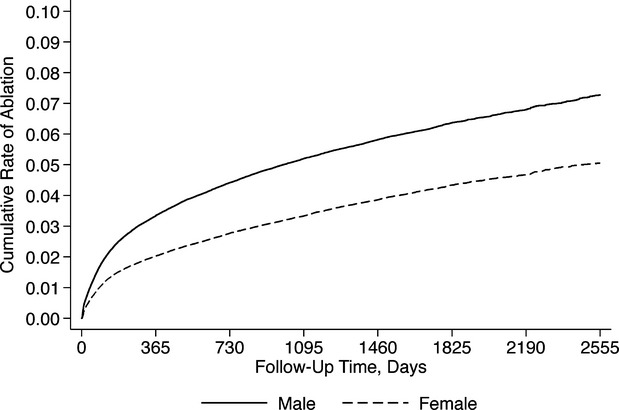
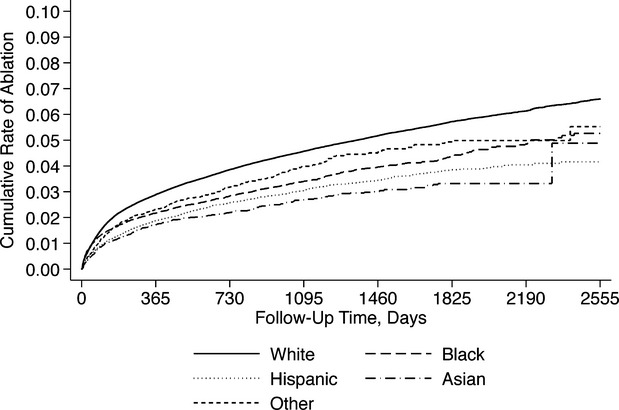
We used data on all admissions at nonfederal acute care hospitals in California, Florida, and New York to identify patients discharged with a primary diagnosis of AF between 2006 and 2011. Our primary outcome was readmission for catheter ablation of AF, identified using validated International Classification of Diseases, Ninth Revision, Clinical Modification procedure codes. Cox regression models were used to assess relationships between demographic characteristics and catheter ablation, adjusting for Elixhauser comorbidities. We identified 397 612 eligible patients. Of these, 16 717 (4.20%, 95% CI 0.41 to 0.43) underwent ablation. These patients were significantly younger, more often male, more often white, and more often privately insured, with higher household incomes and lower rates of medical comorbidity. In Cox regression models, the likelihood of ablation was lower in women than men (hazard ratio [HR] 0.83; 95% CI 0.80 to 0.86) despite higher rates of AF-related rehospitalization (HR 1.23; 95% CI 1.21 to 1.24). Compared to whites, the likelihood of ablation was lower in Hispanics (HR 0.60; 95% CI 0.56 to 0.64) and blacks (HR 0.68; 95% CI 0.64 to 0.73), even though blacks had only a slightly lower likelihood of AF-related rehospitalization (HR 0.97; 95% CI 0.94 to 0.99) and a higher likelihood of all-cause hospitalization (HR 1.38; 95% CI 1.37 to 1.39). Essentially the same pattern existed in Hispanics.
We found differences in use of catheter ablation for symptomatic AF according to sex and race despite adjustment for available data on demographic characteristics and medical comorbidities.
导管消融术越来越多地用于有症状心房颤动(AF)的节律控制,但接受该手术患者的人口统计学特征尚不清楚。
我们利用加利福尼亚州、佛罗里达州和纽约州非联邦急症护理医院的所有入院数据,确定2006年至2011年间以AF为主要诊断出院的患者。我们的主要结局是因AF导管消融再次入院,通过有效的国际疾病分类第九版临床修订版手术编码来确定。采用Cox回归模型评估人口统计学特征与导管消融之间的关系,并对Elixhauser合并症进行校正。我们确定了397612例符合条件的患者。其中,16717例(4.20%,95%CI 0.41至0.43)接受了消融。这些患者明显更年轻,男性更多,白人更多,且更多有私人保险,家庭收入更高,医疗合并症发生率更低。在Cox回归模型中,尽管女性AF相关再住院率较高(风险比[HR]1.23;95%CI 1.21至1.24),但女性接受消融的可能性低于男性(HR 0.83;95%CI 0.80至0.86)。与白人相比,西班牙裔(HR 0.60;95%CI 0.56至0.64)和黑人(HR 0.68;95%CI 0.64至0.73)接受消融的可能性更低,尽管黑人AF相关再住院的可能性仅略低(HR 0.97;95%CI 0.94至0.99),且全因住院的可能性更高(HR 1.38;95%CI 1.37至1.39)。西班牙裔也存在基本相同的模式。
尽管对人口统计学特征和医疗合并症的现有数据进行了校正,但我们发现,根据性别和种族,有症状AF患者在导管消融术的使用上存在差异。