Zeng An, Song Xiaowei, Dong Jiahui, Mitnitski Arnold, Liu Jian, Guo Zhenhui, Rockwood Kenneth
School of Computers, Guangdong University of Technology, Guangzhou, China.
Department of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada. Centre for Healthcare of the Elderly, QEII Health Sciences Centre, Halifax, Nova Scotia, Canada.
J Gerontol A Biol Sci Med Sci. 2015 Dec;70(12):1586-94. doi: 10.1093/gerona/glv084. Epub 2015 Sep 22.
In older adults admitted to intensive care units (ICUs), frailty influences prognosis. We examined the relationship between the frailty index (FI) based on deficit accumulation and early and late survival.
Older patients (≥65 years) admitted to a specialized geriatric ICU at the Liuhuaqiao Hospital, Guangzhou, China between July-December 2011 (n = 155; age 82.7±7.1 y; 87.1% men) were followed for 300 days. The FI was calculated as the proportion present of 52 health deficits. FI performance was compared with that of several prognostic scores.
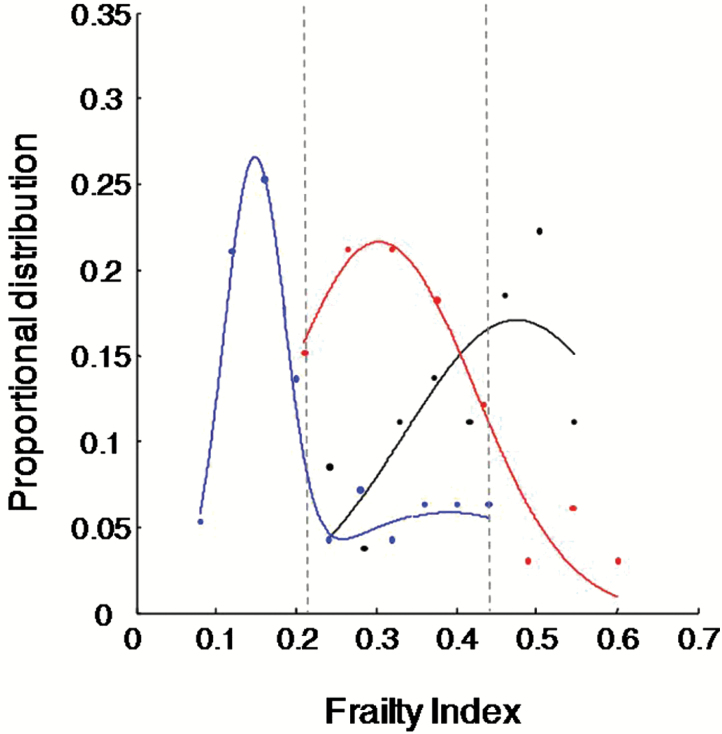
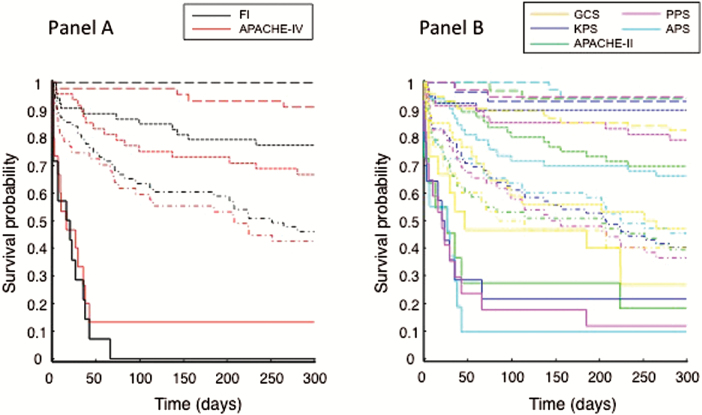
The 90-day death rate was 38.7% (n = 60; 27 died within 30 days). The FI score was correlated with the Glasgow Coma Scale, Karnofsky Scale, Palliative Performance Scale, Acute Physiology Score-APACHE II and APACHE IV (r (2) = 0.52 to 0.72, p < 0.001). Patients who died within 30 days had higher mean FI scores (0.41±0.11) than those who survived to 300 days (0.22±0.11; F = 38.91, p < 0.001). Each 1% increase in the FI from the previous level was associated with an 11% increase in the 30-day mortality risk (95% CI: 7%-15%) adjusting for age, sex, and the prognostic scores. The FI discriminated patients who died in 30 days from those who survived with moderately high accuracy (AUC = 0.89±0.03). No one with an FI score >0.46 survived past 90 days.
ICU survival was strongly associated with the level of frailty at admission. An FI based on health deficit accumulation may help improve critical care outcome prediction in older adults.
在入住重症监护病房(ICU)的老年人中,衰弱会影响预后。我们研究了基于缺陷积累的衰弱指数(FI)与早期和晚期生存之间的关系。
对2011年7月至12月期间在中国广州流花桥医院一家专门的老年ICU住院的老年患者(≥65岁)(n = 155;年龄82.7±7.1岁;男性占87.1%)进行了300天的随访。FI计算为52项健康缺陷的存在比例。将FI的表现与几种预后评分的表现进行比较。
90天死亡率为38.7%(n = 60;27人在30天内死亡)。FI评分与格拉斯哥昏迷量表、卡诺夫斯基量表、姑息治疗表现量表、急性生理评分-APACHE II和APACHE IV相关(r(2)= 0.52至0.72,p < 0.001)。在30天内死亡的患者平均FI评分(0.41±0.11)高于存活至300天的患者(0.22±0.11;F = 38.91,p < 0.001)。在调整年龄、性别和预后评分后,FI较前一水平每增加1%,30天死亡风险增加11%(95%可信区间:7%-15%)。FI以中等高度的准确性区分了在30天内死亡的患者和存活的患者(曲线下面积 = 0.89±0.03)。FI评分>0.46的患者无一人存活超过90天。
ICU生存与入院时的衰弱程度密切相关。基于健康缺陷积累的FI可能有助于改善对老年患者重症监护结局的预测。