Department of Intensive Care, Inselspital Bern University Hospital and University of Bern, Bern, Switzerland.
Deutsches Herzzentrum Berlin, Berlin, Germany.
Gerontology. 2022;68(12):1321-1349. doi: 10.1159/000523674. Epub 2022 Mar 25.
As new treatments have become established, more frail pre-ICU patients are being admitted to intensive care units (ICUs); this is creating new challenges to provide adequate care and to ensure that resources are allocated in an ethical and economical manner. This systematic review evaluates the current standard for assessing frailty on the ICU, including methods of assessment, time point of measurements, and cut-offs.
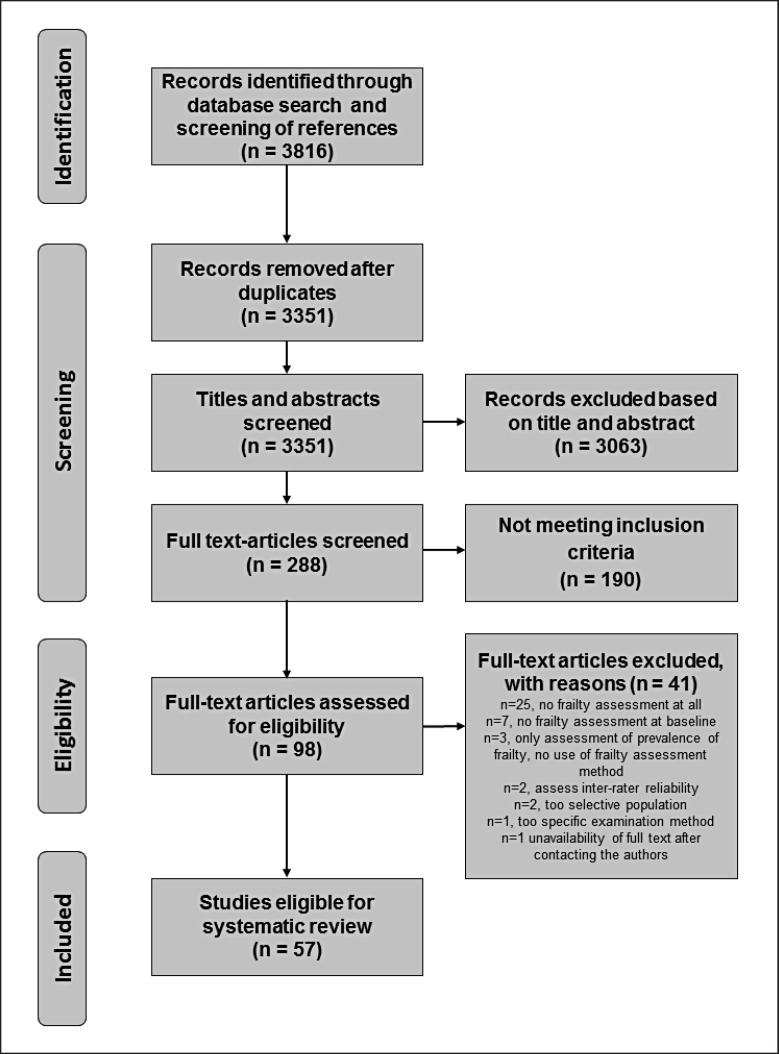
A systematic search was conducted on MEDLINE, Clinical Trials, Cochrane Library, and Embase. Randomized and non-randomized controlled studies were included that evaluated diagnostic tools and ICU outcomes for frailty. Exclusion criteria were the following: studies without baseline assessment of frailty on ICU admission, studies in paediatric patients or pregnant women, and studies that targeted very narrow populations of ICU patients. Eligible articles were included until January 31, 2021. Methodological quality was assessed using the Newcastle-Ottawa Scale. No meta-analysis was performed, due to heterogeneity.
N = 57 articles (253,376 patients) were included using 19 different methods to assess frailty or a surrogate. Frailty on ICU admission was most frequently detected using the Clinical Frailty Scale (CFS) (n = 35, 60.3%), the Frailty Index (n = 5, 8.6%), and Fried's frailty phenotype (n = 6, 10.3%). N = 22 (37.9%) studies assessed functional status. Cut-offs, time points, and manner of baseline assessment of frailty on ICU admission varied widely. Frailty on ICU admission was associated with short- and long-term mortality, functional and cognitive impairment, increased health care dependency, and impaired quality of life post-ICU discharge.
Frailty assessment on the ICU is heterogeneous with respect to methods, cut-offs, and time points. The CFS may best reflect frailty in the ICU. Frailty assessments should be harmonized and performed routinely in the critically ill.
随着新的治疗方法得到确立,更多身体虚弱的 ICU 前患者被收治到重症监护病房(ICU);这给提供充分的护理以及确保以合乎道德和经济的方式分配资源带来了新的挑战。本系统评价评估了 ICU 中目前评估脆弱性的标准,包括评估方法、测量时间点和截止值。
对 MEDLINE、临床试验、Cochrane 图书馆和 Embase 进行了系统检索。纳入了评估脆弱性诊断工具和 ICU 结局的随机和非随机对照研究。排除标准为:无 ICU 入院时基线脆弱性评估的研究、儿科患者或孕妇的研究,以及针对 ICU 患者非常狭窄人群的研究。合格的文章纳入截止到 2021 年 1 月 31 日。使用纽卡斯尔-渥太华量表评估方法学质量。由于异质性,未进行荟萃分析。
共纳入 57 篇文章(253376 例患者),使用 19 种不同的方法评估脆弱性或替代指标。最常使用临床虚弱量表(CFS)(n=35,60.3%)、虚弱指数(n=5,8.6%)和 Fried 虚弱表型(n=6,10.3%)检测 ICU 入院时的虚弱。n=22(37.9%)的研究评估了功能状态。ICU 入院时脆弱性的截止值、时间点和基线评估方式差异很大。ICU 入院时的虚弱与短期和长期死亡率、功能和认知障碍、增加的医疗保健依赖以及 ICU 出院后的生活质量受损有关。
ICU 中脆弱性评估在方法、截止值和时间点方面存在差异。CFS 可能最能反映 ICU 中的脆弱性。应协调脆弱性评估并在危重病患者中常规进行。