Poe Stacy, Vandivier-Pletsch Robin H, Clay Michael, Wong Hector R, Haynes Erin, Rothenberg Florence G
From the *Department of Veterans Affairs, Office of Informatics and Analytics, Office of Productivity, Efficiency and Staffing; †Cardiology Division, Department of Internal Medicine, Cincinnati Veterans Administration Medical Center; ‡Division of Cardiovascular Health and Disease, Department of Internal Medicine, University of Cincinnati; §Division of Critical Care Medicine, Department of Pediatrics, Cincinnati Children's Hospital Medical Center; and ∥Department of Environmental Health, University of Cincinnati, Cincinnati, OH.
J Investig Med. 2015 Dec;63(8):905-15. doi: 10.1097/JIM.0000000000000239.
Elevated cardiac troponin (cTn) in the absence of acute coronary syndromes (ACS) is associated with increased mortality in critically ill patients. There are no evidence-based interventions that reduce mortality in this group.
We performed a retrospective investigation of the Veterans Administration Inpatient Evaluation Center database to determine whether drugs used in ACS (β-blockers, aspirin, and statins) are associated with reduced mortality in critically ill patients.
Thirty-day mortality was determined for non-ACS patients admitted to any Veterans Administration Intensive Care Unit between October 1, 2007, and September 30, 2008, adjusted for severity of illness. Troponin assay values were normalized across institutions.
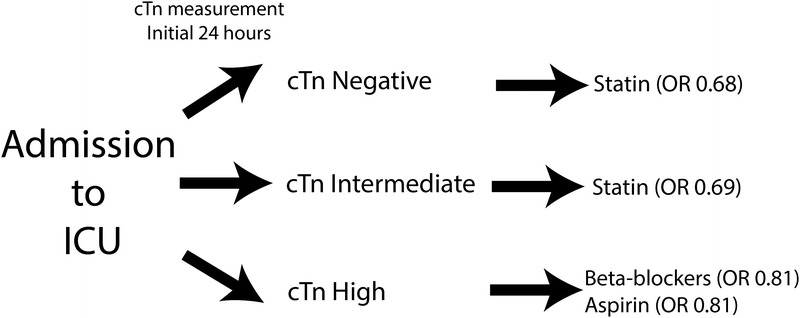
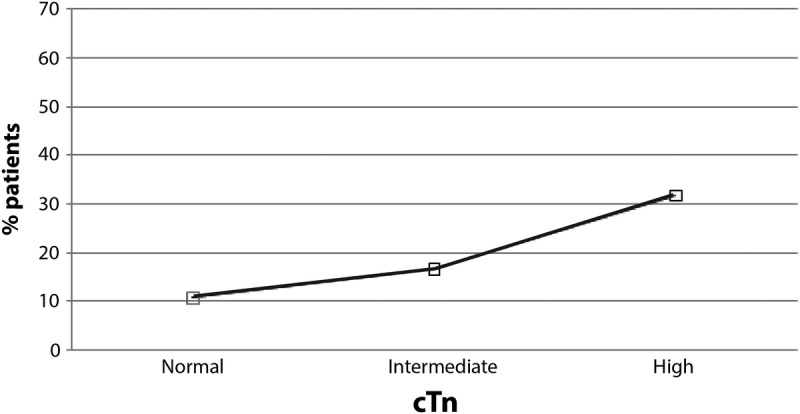
Multivariate analyses for 30-day mortality showed an odds ratio (OR) of 1.82 for patients with high cTn (P < 0.0001, cTn > 10% coefficient of variation) and 1.18 for intermediate cTn (P = 0.0021, cTn between lowest limit detectable and 10% coefficient of variation) compared with patients with no elevation, adjusting for severity of illness (n = 19,979). Logistic regression models showed that patients with no or intermediate elevations of cTn taking statins within 24 hours of cTn measurement had a lower mortality than patients not taking statins (OR, 0.66; 95% confidence interval [95% CI], 0.53-0.82; P = 0.0003), whereas patients with high cTn had a lower mortality if they were taking β-blockers or aspirin within 24 hours of cTn measurement compared to patients not taking β-blockers or aspirin (β-blockers: OR, 0.80; 95% CI, 0.68-0.94; P = 0.0077; aspirin: OR, 0.81;95% CI, 0.69-0.96; P = 0.0134).
This retrospective study confirms an association between elevated troponin and outcomes in critically ill patients without ACS and identifies statins, β-blockers, and aspirin as potential outcome modifiers in a cTn-dependent manner.
在无急性冠状动脉综合征(ACS)的情况下,心脏肌钙蛋白(cTn)升高与危重症患者死亡率增加相关。目前尚无基于证据的干预措施可降低该组患者的死亡率。
我们对退伍军人事务部住院患者评估中心数据库进行了一项回顾性调查,以确定ACS中使用的药物(β受体阻滞剂、阿司匹林和他汀类药物)是否与危重症患者死亡率降低相关。
确定2007年10月1日至2008年9月30日期间入住任何退伍军人事务部重症监护病房的非ACS患者的30天死亡率,并根据疾病严重程度进行调整。肌钙蛋白检测值在各机构间进行了标准化。
对30天死亡率的多变量分析显示,与未升高的患者相比,高cTn患者(P<0.0001,cTn>变异系数10%)的比值比(OR)为1.82,中度cTn患者(P = 0.0021,cTn在最低可检测限与变异系数10%之间)的OR为1.18,对疾病严重程度进行了校正(n = 19979)。逻辑回归模型显示,在cTn测量后24小时内服用他汀类药物的cTn无升高或中度升高的患者,其死亡率低于未服用他汀类药物的患者(OR,0.66;95%置信区间[95%CI],0.53 - 0.82;P = 0.0003),而高cTn患者在cTn测量后24小时内服用β受体阻滞剂或阿司匹林时,其死亡率低于未服用β受体阻滞剂或阿司匹林的患者(β受体阻滞剂:OR,0.80;95%CI,0.68 - 0.94;P = 0.0077;阿司匹林:OR,0.81;95%CI,0.69 - 0.96;P = 0.0134)。
这项回顾性研究证实了在无ACS的危重症患者中肌钙蛋白升高与预后之间的关联,并确定他汀类药物、β受体阻滞剂和阿司匹林是以cTn依赖的方式作为潜在的预后改善因素。