Department of Internal Medicine, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania.
Division of Cardiology, Rush University Medical Center, Chicago, Illinois.
Cardiovasc Pathol. 2021 Nov-Dec;55:107374. doi: 10.1016/j.carpath.2021.107374. Epub 2021 Aug 3.
The variability of coronavirus disease 2019 (COVID-19) illness severity has puzzled clinicians and has sparked efforts to better predict who would benefit from rapid intervention. One promising biomarker for in-hospital morbidity and mortality is cardiac troponin (cTn).
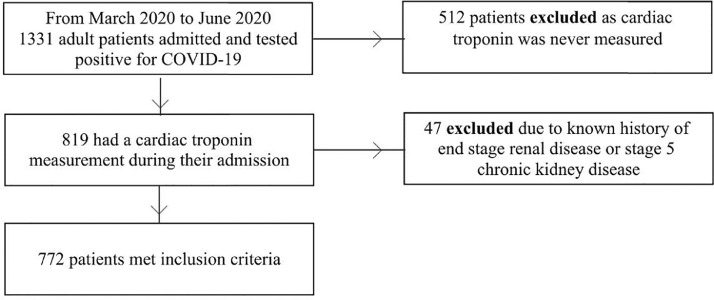
A retrospective study of 1331 adult patients with COVID-19 admitted to the Rush University System in Illinois, USA was performed. Patients without cTn measurement during their admission or a history of end stage renal disease or stage 5 chronic kidney disease were excluded. Using logistic regression adjusted for baseline characteristics, pre-existing comorbidities, and other laboratory markers of inflammation, cTn was assessed as a predictor of 60-day mortality and severe COVID-19 infection, consisting of a composite of 60-day mortality, need for intensive care unit, or requiring non-invasive positive pressure ventilation or intubation.
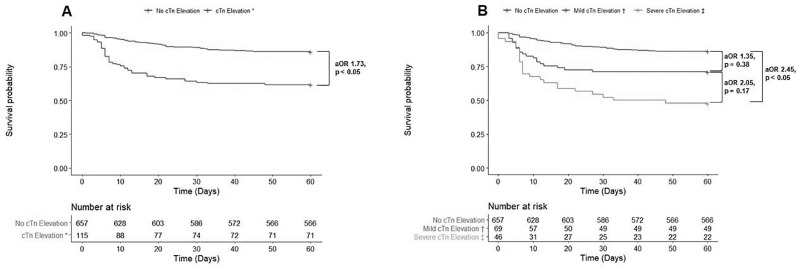
A total of 772 patients met inclusion criteria. Of these, 69 (8.9%) had mild cTn elevation (> 1 to < 2x upper limit of normal (ULN)) and 46 (6.0%) had severe cTn elevation (≥ 2x ULN). Regardless of baseline characteristics, comorbidities, and initial c-reactive protein, lactate dehydrogenase, and ferritin, when compared to the normal cTn group, mild cTn elevation and severe cTn elevation were predictors of severe COVID-19 infection (adjusted OR [aOR] aOR 3.00 [CI: 1.51 - 6.29], P < 0.01; aOR 9.96 [CI: 2.75 - 64.23], P < 0.01, respectively); severe cTn elevation was a predictor of in-hospital mortality (aOR 2.42 [CI: 1.10 - 5.21], P < 0.05) and 60-day mortality (aOR 2.45 [CI: 1.13 - 5.25], P < 0.05).
In our cohort, both mild and severe initial cTn elevation were predictors of severe COVID-19 infection, while only severe cTn elevation was predictive of 60-day mortality. First cTn value on hospitalization is a valuable longitudinal prognosticator for COVID-19 disease severity and mortality.
新型冠状病毒病 2019(COVID-19)疾病严重程度的变化令临床医生感到困惑,并促使人们努力更好地预测谁将受益于快速干预。心脏肌钙蛋白(cTn)是住院发病率和死亡率的一个有前途的生物标志物。
对美国伊利诺伊州拉什大学系统收治的 1331 例成年 COVID-19 患者进行回顾性研究。排除入院时未测量 cTn 或有终末期肾病或 5 期慢性肾脏病病史的患者。使用调整基线特征、预先存在的合并症和其他炎症实验室标志物的逻辑回归,评估 cTn 作为 60 天死亡率和严重 COVID-19 感染的预测指标,严重 COVID-19 感染包括 60 天死亡率、需要重症监护、需要无创正压通气或插管的复合指标。
共有 772 例患者符合纳入标准。其中,69 例(8.9%)有轻度 cTn 升高(> 1 至< 2x 正常值上限(ULN)),46 例(6.0%)有重度 cTn 升高(≥ 2x ULN)。无论基线特征、合并症和初始 C 反应蛋白、乳酸脱氢酶和铁蛋白如何,与正常 cTn 组相比,轻度 cTn 升高和重度 cTn 升高均为严重 COVID-19 感染的预测指标(调整后的比值比[OR]aOR 3.00[CI:1.51-6.29],P<0.01;aOR 9.96[CI:2.75-64.23],P<0.01);重度 cTn 升高是住院死亡率(aOR 2.42[CI:1.10-5.21],P<0.05)和 60 天死亡率(aOR 2.45[CI:1.13-5.25],P<0.05)的预测指标。
在我们的队列中,轻度和重度初始 cTn 升高均为严重 COVID-19 感染的预测指标,而只有重度 cTn 升高可预测 60 天死亡率。入院时的首次 cTn 值是 COVID-19 疾病严重程度和死亡率的有价值的纵向预测指标。