Oda Hitomi, Miyauchi Akira, Ito Yasuhiro, Yoshioka Kana, Nakayama Ayako, Sasai Hisanori, Masuoka Hiroo, Yabuta Tomonori, Fukushima Mitsuhiro, Higashiyama Takuya, Kihara Minoru, Kobayashi Kaoru, Miya Akihiro
1 Department of Surgery, Kuma Hospital, Kobe , Japan .
2 Clinical Trial Management Center, Kuma Hospital, Kobe , Japan .
Thyroid. 2016 Jan;26(1):150-5. doi: 10.1089/thy.2015.0313. Epub 2015 Nov 5.
The incidence of papillary microcarcinoma (PMC) of the thyroid is rapidly increasing globally, making the management of PMC an important clinical issue. Excellent oncological outcomes of active surveillance for low-risk PMC have been reported previously. Here, unfavorable events following active surveillance and surgical treatment for PMC were studied.
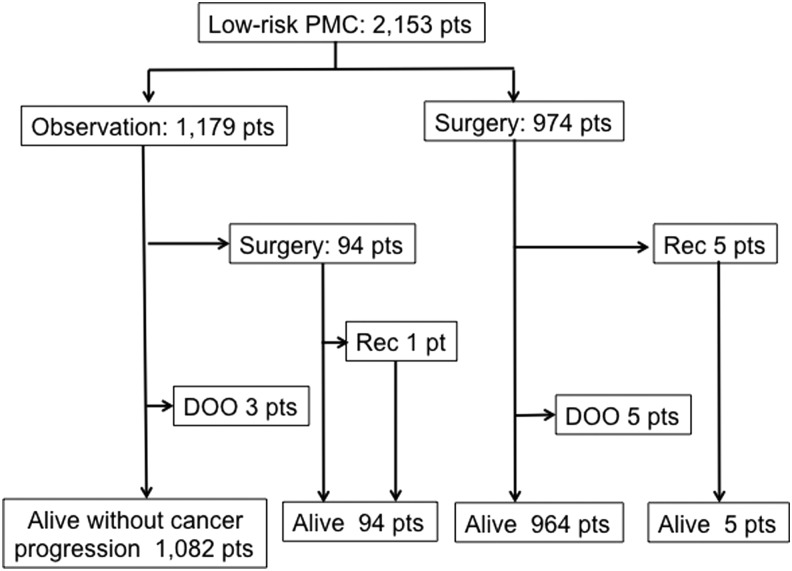
From February 2005 to August 2013, 2153 patients were diagnosed with low-risk PMC. Of these, 1179 patients chose active surveillance and 974 patients chose immediate surgery. The oncological outcomes and the incidences of unfavorable events of these groups were analyzed.
In the active surveillance group, 94 patients underwent surgery for various reasons; tumor enlargement and the appearance of novel lymph node metastases were the reasons in 27 (2.3%) and six patients (0.5%), respectively. One of the patients with conversion to surgery had nodal recurrence, and five patients in the immediate surgery group had a recurrence in a cervical node or unresected thyroid lobe. All of these recurrences were successfully treated. None of the patients had distant metastases, and none died of the disease. The immediate surgery group had significantly higher incidences of transient vocal cord paralysis (VCP), transient hypoparathyroidism, and permanent hypoparathyroidism than the active-surveillance group did (4.1% vs. 0.6%, p < 0.0001; 16.7% vs. 2.8%, p < 0.0001; and 1.6% vs. 0.08%, p < 0.0001, respectively). Permanent VCP occurred only in two patients (0.2%) in the immediate surgery group. The proportion of patients on L-thyroxine for supplemental or thyrotropin (TSH)-suppressive purposes was significantly larger in the immediate surgery group than in the active surveillance group (66.1% vs. 20.7%, p < 0.0001). The immediate surgery group had significantly higher incidences of postsurgical hematoma and surgical scar in the neck compared with the active surveillance group (0.5% vs. 0%, p < 0.05; and 8.0% vs. 100%, p < 0.0001, respectively).
The oncological outcomes of the immediate surgery and active surveillance groups were similarly excellent, but the incidences of unfavorable events were definitely higher in the immediate surgery group. Thus, active surveillance is now recommended as the best choice for patients with low-risk PMC.
甲状腺微小乳头状癌(PMC)的发病率在全球范围内迅速上升,使得PMC的管理成为一个重要的临床问题。此前已有报道称,对低风险PMC进行主动监测可获得良好的肿瘤学结果。在此,我们对PMC主动监测和手术治疗后的不良事件进行了研究。
2005年2月至2013年8月,2153例患者被诊断为低风险PMC。其中,1179例患者选择主动监测,974例患者选择立即手术。分析了这些组的肿瘤学结果和不良事件发生率。
在主动监测组中,94例患者因各种原因接受了手术;肿瘤增大和出现新的淋巴结转移分别是27例(2.3%)和6例患者(0.5%)的原因。转为手术的患者中有1例出现淋巴结复发,立即手术组中有5例患者在颈部淋巴结或未切除的甲状腺叶出现复发。所有这些复发均得到成功治疗。所有患者均无远处转移,也无患者死于该疾病。立即手术组的短暂性声带麻痹(VCP)、短暂性甲状旁腺功能减退和永久性甲状旁腺功能减退的发生率显著高于主动监测组(分别为4.1%对0.6%,p < 0.0001;16.7%对2.8%,p < 0.0001;1.6%对0.08%,p < 0.0001)。永久性VCP仅发生在立即手术组的2例患者(0.2%)中。立即手术组中因补充或促甲状腺激素(TSH)抑制目的而服用左甲状腺素的患者比例显著高于主动监测组(66.1%对20.7%,p < 0.0001)。与主动监测组相比,立即手术组术后颈部血肿和手术瘢痕的发生率显著更高(分别为0.5%对0%,p < 0.05;8.0%对100%,p < 0.0001)。
立即手术组和主动监测组的肿瘤学结果同样出色,但立即手术组的不良事件发生率肯定更高。因此,目前建议主动监测作为低风险PMC患者的最佳选择。