Luijks Hilde, Biermans Marion, Bor Hans, van Weel Chris, Lagro-Janssen Toine, de Grauw Wim, Schermer Tjard
Department of Primary and Community Care, Radboud university medical center, Nijmegen, The Netherlands.
Department of Primary and Community Care, Radboud university medical center, Nijmegen, The Netherlands; Australian Primary Health Care Research Institute, Australian National University, Canberra, Australia.
PLoS One. 2015 Oct 1;10(10):e0138662. doi: 10.1371/journal.pone.0138662. eCollection 2015.
To explore the longitudinal effect of chronic comorbid diseases on glycemic control (HbA1C) and systolic blood pressure (SBP) in type 2 diabetes patients.
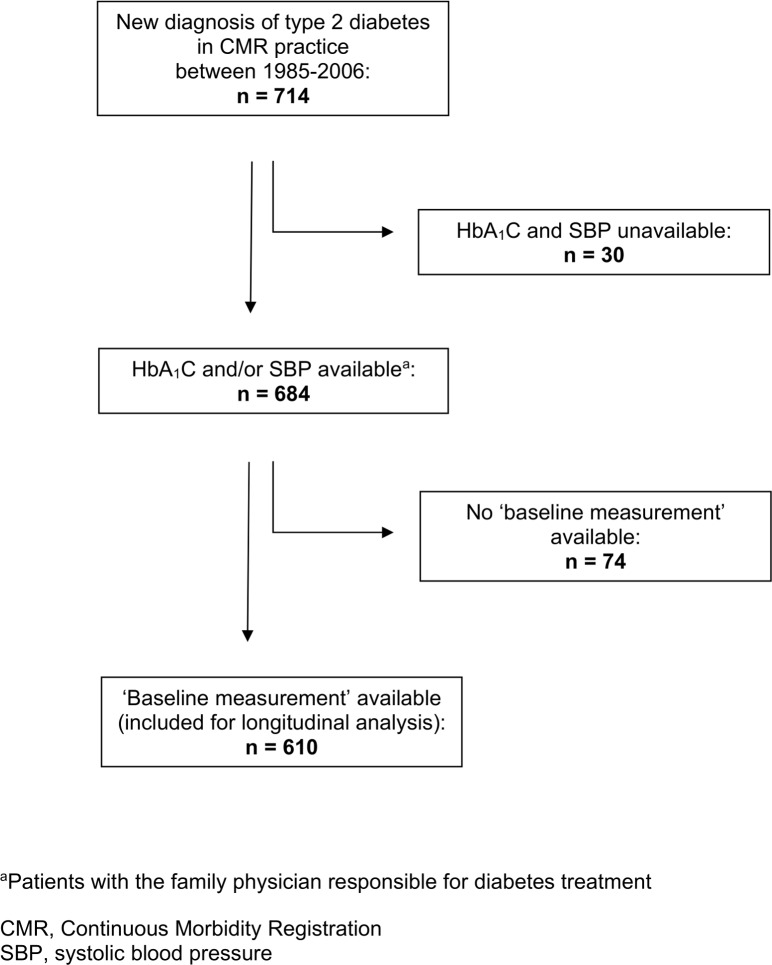
In a representative primary care cohort of patients with newly diagnosed type 2 diabetes in The Netherlands (n = 610), we tested differences in the five year trend of HbA1C and SBP according to comorbidity profiles. In a mixed model analysis technique we corrected for relevant covariates. Influence of comorbidity (a chronic disease already present when diabetes was diagnosed) was tested as total number of comorbid diseases, and as presence of specific disease groups, i.e. cardiovascular, mental, and musculoskeletal disease, malignancies, and COPD. In subgroup effect analyses we tested if potential differences were modified by age, sex, socioeconomic status, and BMI.
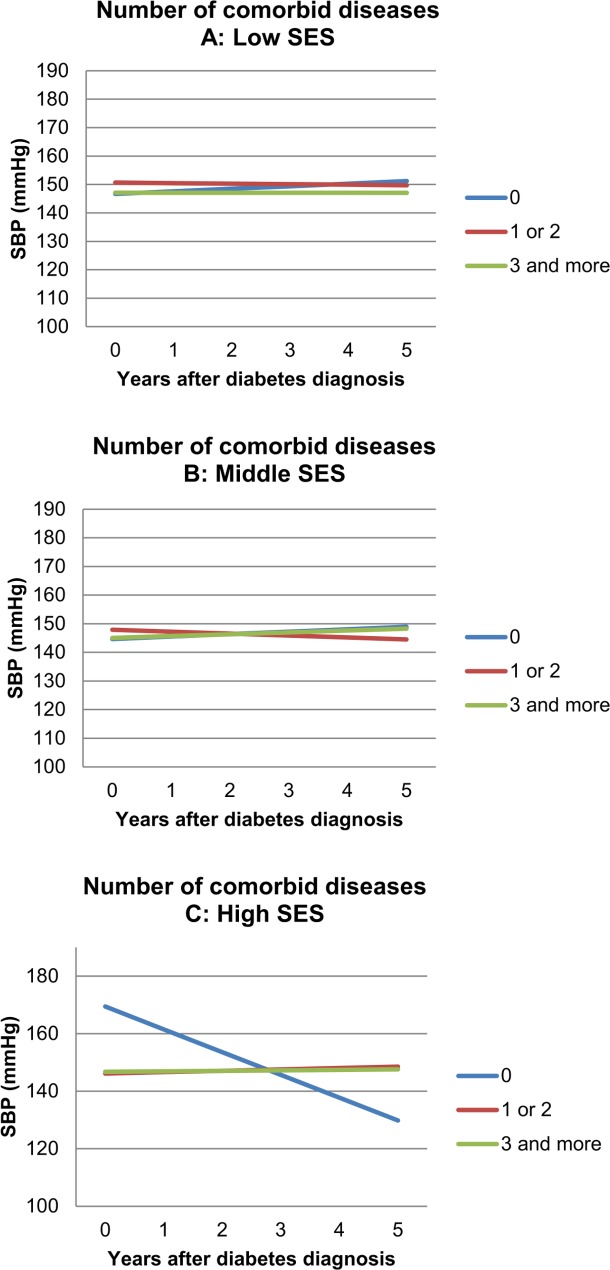
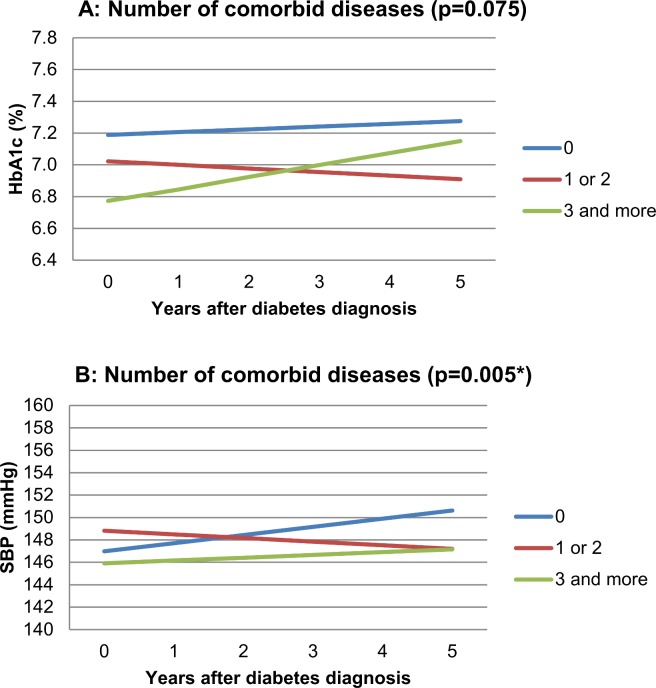
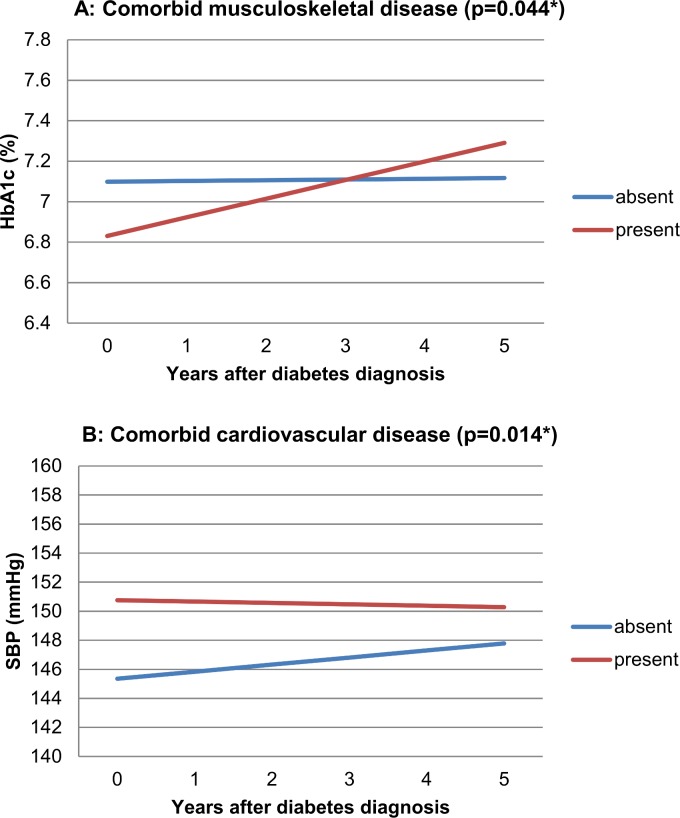
The number of comorbid diseases significantly influenced the SBP trend, with highest values after five years for diabetes patients without comorbidity (p = 0.005). The number of diseases did not influence the HbA1C trend (p = 0.075). Comorbid musculoskeletal disease resulted in lower HbA1C at the time of diabetes diagnosis, but in higher values after five years (p = 0.044). Patients with cardiovascular diseases had sustained elevated levels of SBP (p = 0.014). Effect modification by socioeconomic status was observed in some comorbidity subgroups.
Presence of comorbidity in type 2 diabetes patients affected the long-term course of HbA1C and SBP in this primary care cohort. Numbers and types of comorbidity showed differential effects: not the simple sum of diseases, but specific types of comorbid disease had a negative influence on long-term diabetes control parameters. The complex interactions between comorbidity, diabetes control and effect modifiers require further investigation and may help to personalize treatment goals.
探讨慢性合并症对2型糖尿病患者血糖控制(糖化血红蛋白[HbA1C])和收缩压(SBP)的纵向影响。
在荷兰一个具有代表性的新诊断2型糖尿病患者初级保健队列(n = 610)中,我们根据合并症情况测试了HbA1C和SBP五年趋势的差异。在混合模型分析技术中,我们对相关协变量进行了校正。将合并症(糖尿病诊断时已存在的慢性疾病)的影响作为合并疾病的总数以及特定疾病组(即心血管疾病、精神疾病、肌肉骨骼疾病、恶性肿瘤和慢性阻塞性肺疾病[COPD])的存在情况进行测试。在亚组效应分析中,我们测试了年龄、性别、社会经济地位和体重指数(BMI)是否会改变潜在差异。
合并疾病的数量显著影响SBP趋势,无合并症的糖尿病患者五年后的SBP值最高(p = 0.005)。疾病数量未影响HbA1C趋势(p = 0.075)。合并肌肉骨骼疾病在糖尿病诊断时导致较低的HbA1C,但五年后升高(p = 0.044)。心血管疾病患者的SBP持续升高(p = 0.014)。在一些合并症亚组中观察到社会经济地位的效应修正。
2型糖尿病患者合并症的存在影响了该初级保健队列中HbA1C和SBP的长期病程。合并症的数量和类型显示出不同的影响:不是疾病的简单总和,而是特定类型的合并疾病对长期糖尿病控制参数有负面影响。合并症、糖尿病控制和效应修饰因素之间的复杂相互作用需要进一步研究,可能有助于实现治疗目标的个性化。