Department of Medicine Quality Program.
Divisions of Rheumatology, Immunology and Allergy.
Open Forum Infect Dis. 2015 Oct 1;2(4):ofv119. doi: 10.1093/ofid/ofv119. eCollection 2015 Dec.
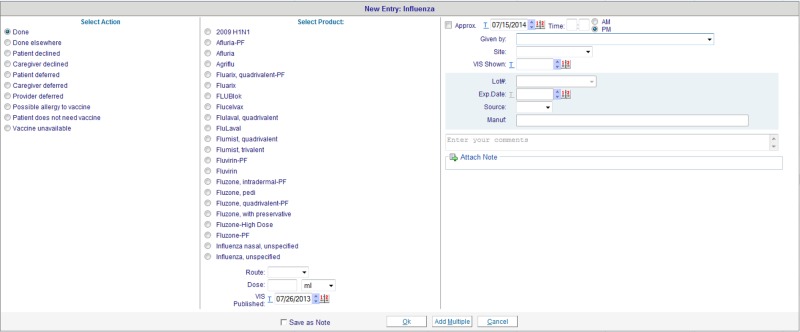
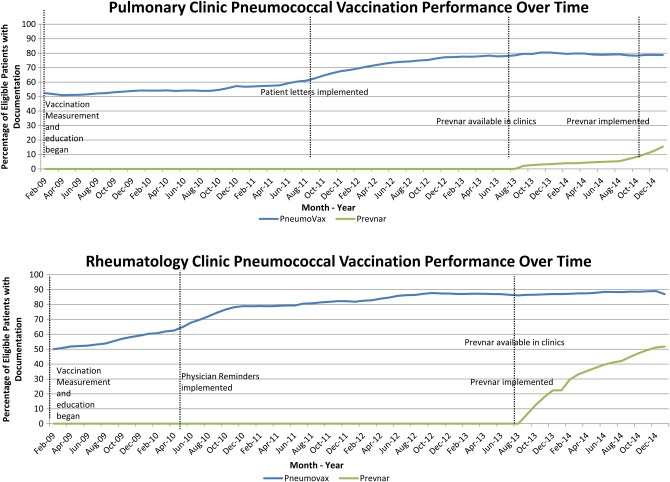
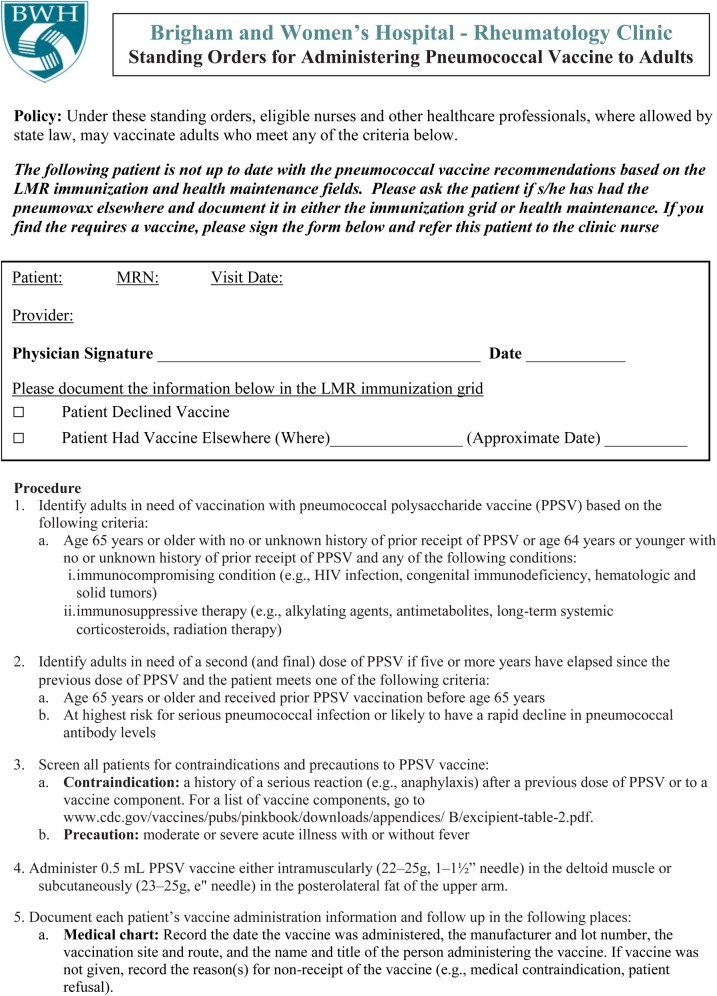
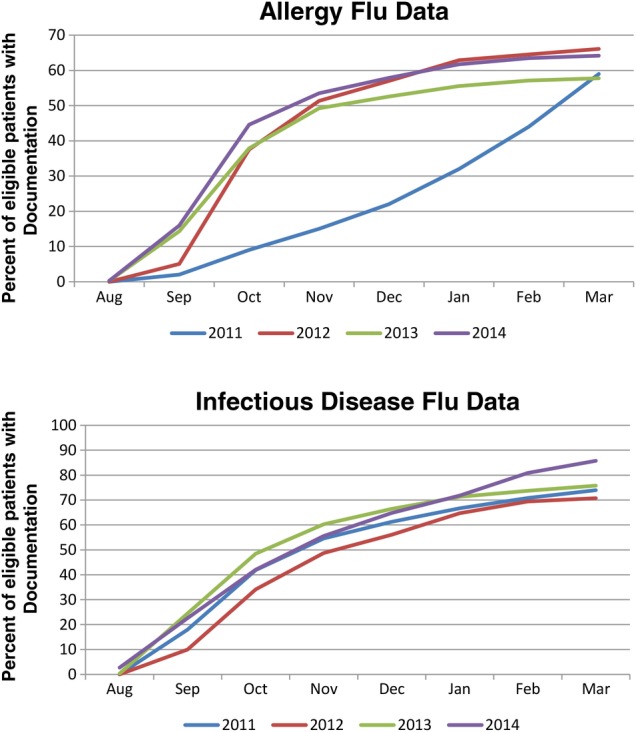
Background. Influenza and pneumococcal vaccinations are recommended for elderly and high-risk patients; however, rates of adherence are low. We sought to implement influenza and pneumococcal vaccine initiatives in 4 different ambulatory specialty practices, using 3 unique approaches. Methods. Four specialties with high-risk patient populations were selected for intervention: allergy (asthma), infectious disease (ID) (human immunodeficiency virus), pulmonary (chronic lung disease), and rheumatology (immunocompromised). Allergy and ID focused on influenza vaccination, and pulmonary and rheumatology focused on pneumococcal vaccination. We used 3 strategies for quality improvement: physician reminders, patient letters, and a nurse-driven model. Physicians were provided their performance data on a monthly basis and presented trended data on a quarterly basis at staff meetings. Results. All 4 specialties developed processes for improving vaccination rates with all showing some increase. Higher rates were achieved with pneumococcal vaccine than influenza. Pneumococcal vaccine rates showed steady improvement from year to year while influenza vaccine rates remained relatively constant. Allergy's influenza rate was 59% in 2011 and 64% in the 2014 flu season. Infectious disease influenza rates moved from 74% in the 2011 flu season to 86% for the 2014 season. Pneumococcal vaccine in pulmonary patients' rate was 52% at the start of intervention in February 2009 and 79% as of January 2015. Rheumatology rates rose from 50% in February 2009 to 87% in January 2015. Conclusions. Integrated routine workflow and performance data sharing can effectively engage specialists and staff in vaccine adherence improvement. Influenza vaccination may require other approaches to achieve the rates seen with pneumococcal vaccine.
流感和肺炎球菌疫苗推荐用于老年和高危患者;然而,其接种率很低。我们试图在 4 个不同的门诊专科诊所实施流感和肺炎球菌疫苗接种计划,采用 3 种不同的方法。方法:选择具有高危患者人群的 4 个专科进行干预:过敏(哮喘)、传染病(艾滋病病毒)、肺病和风湿病(免疫功能低下)。过敏和传染病专注于流感疫苗接种,而肺病和风湿病则专注于肺炎球菌疫苗接种。我们使用 3 种策略来进行质量改进:医生提醒、患者信函和护士主导模式。医生每月收到他们的绩效数据,并在员工会议上每季度呈现趋势数据。结果:所有 4 个专科都制定了提高疫苗接种率的流程,所有专科的接种率都有所提高。肺炎球菌疫苗的接种率高于流感疫苗。肺炎球菌疫苗的接种率逐年稳步提高,而流感疫苗的接种率则相对稳定。过敏的流感疫苗接种率从 2011 年的 59%提高到 2014 年流感季节的 64%。传染病的流感疫苗接种率从 2011 年流感季节的 74%提高到 2014 年的 86%。肺病患者的肺炎球菌疫苗接种率在 2009 年 2 月开始干预时为 52%,截至 2015 年 1 月为 79%。风湿病的接种率从 2009 年 2 月的 50%上升到 2015 年 1 月的 87%。结论:整合常规工作流程和绩效数据共享可以有效地让专家和工作人员参与到疫苗接种的改进中来。流感疫苗接种可能需要采取其他方法来达到肺炎球菌疫苗接种的效果。