Gander Jennifer C, Sui Xuemei, Hébert James R, Hazlett Linda J, Cai Bo, Lavie Carl J, Blair Steven N
Department of Surgery, School of Medicine, Emory University, Atlanta, GA.
Department of Exercise Science, Arnold School of Public Health, University of South Carolina, Columbia.
Mayo Clin Proc. 2015 Oct;90(10):1372-9. doi: 10.1016/j.mayocp.2015.07.017.
To examine the association of cardiorespiratory fitness (CRF) with risk of coronary heart disease (CHD) while controlling for an individual's Framingham Risk Score (FRS)-predicted CHD risk.
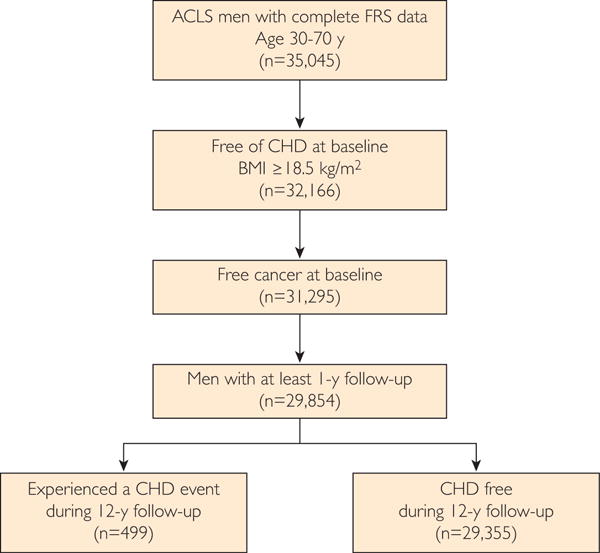
The study included 29,854 men from the Aerobics Center Longitudinal Study, who received a baseline examination from January 1, 1979, to December 31, 2002. Coronary heart disease events included self-reported myocardial infarction or revascularization or CHD death. Multivariable survival analysis investigated the association between CRF, FRS, and CHD. Cardiorespiratory fitness was analyzed as both a continuous and a categorical variable. The population was stratified by "low" and "moderate or high" risk of CHD to test for differences in the FRS stratified by CRF.
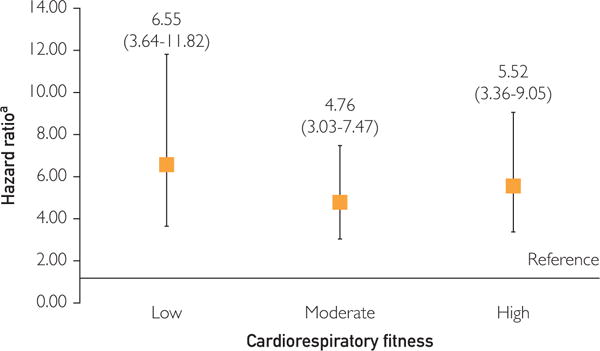
Compared with men without incident CHD, men with incident CHD were older (mean age, 51.6 years vs 44.6 years), had lower average maximally achieved fitness (10.9 metabolic equivalent of tasks vs 12.0 metabolic equivalent of tasks [METs]), and were more likely to have moderate or high 10-year CHD risk (P<.001). Cardiorespiratory fitness, defined as maximal METs, exhibited a 20% lower risk of CHD (hazard ratio, 0.80; 95% CI, 0.77-0.83) for each 1-unit MET increase. Among men in the low CRF strata, individuals with moderate or high 10-year CHD risk, according to the FRS, had a higher CHD risk (hazard ratio, 6.55; 95% CI, 3.64-11.82) than men with low CHD risk according to the FRS.
Clinicians should promote physical activity to improve CRF so as to reduce CHD risk, even to patients with otherwise low CHD risk.
在控制个体弗雷明汉风险评分(FRS)预测的冠心病风险的同时,研究心肺适能(CRF)与冠心病(CHD)风险之间的关联。
该研究纳入了来自有氧运动中心纵向研究的29854名男性,他们在1979年1月1日至2002年12月31日期间接受了基线检查。冠心病事件包括自我报告的心肌梗死或血运重建或冠心病死亡。多变量生存分析研究了CRF、FRS与冠心病之间的关联。心肺适能被分析为连续变量和分类变量。根据冠心病“低”风险和“中或高”风险对人群进行分层,以检验按CRF分层的FRS差异。
与无冠心病事件的男性相比,有冠心病事件的男性年龄更大(平均年龄,51.6岁对44.6岁),平均最大运动能力更低(10.9代谢当量对12.0代谢当量[METs]),且更有可能有中度或高度的10年冠心病风险(P<0.001)。以最大METs定义的心肺适能,每增加1个单位的MET,冠心病风险降低20%(风险比,0.80;95%CI,0.77 - 0.83)。在低CRF分层的男性中,根据FRS有中度或高度10年冠心病风险的个体,其冠心病风险(风险比,6.55;95%CI,3.64 - 11.82)高于根据FRS有低冠心病风险的男性。
临床医生应促进体育活动以提高CRF,从而降低冠心病风险,即使是对那些原本冠心病风险较低的患者。