El Hammoumi Mohammed Massine, Slaoui Omar, El Oueriachi Fayçal, Kabiri El Hassane
Department of Thoracic Surgery, Mohamed V Military University Hospital, Riad 10100, Rabat, Morocco.
Center of doctoral studies, Faculty of Medecine and Pharmacy, Mohamed V University, Rabat, Morocco.
BMC Surg. 2015 Oct 16;15:114. doi: 10.1186/s12893-015-0103-4.
This study was conducted to determine the efficacy of surgery in the treatment of complex aspergilloma comparatively with simple aspergilloma.
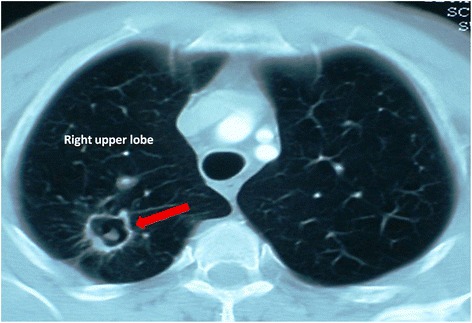
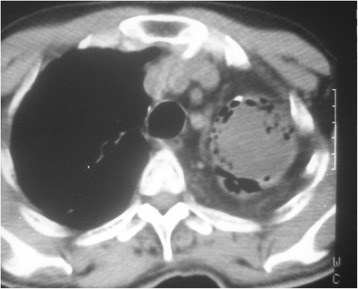
From January 2006 to December 2014, 115 cases of pulmonary aspergilloma were admitted in our department. One operation on one side was counted as one case and the patients were divided into two groups. In group A: 61 cases of complex aspergilloma. In group B: 50 patients underwent 54 cases of lung resection for simple aspergilloma. People who underwent arteriography and embolization were excluded. Surgical treatment was indicated when 1) recurrent aspergilloma-related hemoptysis, 2) definite simple or complex aspergilloma and 3) a simultaneous bilateral aspergilloma.
People with complex aspergilloma were big smokers with lower BMI, and had reduced lung function parameters. The main symptoms were repeated hemoptysis, chronic cough, abundant purulent expectoration and respiratory infections. Lobectomy was the most performed indication. In group B, number of wedge resections was larger than group A with statistical significant difference (p = 0.001). In the post-operative course morbidity was higher in group A (16%) vs (9%) in group B with statistical difference (p = 0.026). The median follow-up was 30 months (range 19-52 months). The median duration of chest tube drainage was 4 days. The duration of chest tube drainage was longer in the group A (4.7 ± 1.4 versus 2.9 ± 1.3; p = 0.005). The prolonged postoperative air leakage occurred more frequently in group A (14.75%; versus 1.8% p = 0.015). In group A, 3 cases and 2 in group B underwent a secondary operation for post operative hemothorax. Bronchopleural fistula occurred exclusively in group A (n = 4).
The surgical resection should be used in a multidisciplinary approach. Preoperative Interventional therapies could optimize the conditions for the operation. Total surgical resection must be the treatment of choice of localized causative lesions.
本研究旨在比较手术治疗复杂性曲菌球与单纯性曲菌球的疗效。
2006年1月至2014年12月,我科收治115例肺曲菌球患者。一侧行一次手术计为1例,将患者分为两组。A组:61例复杂性曲菌球。B组:50例患者因单纯性曲菌球行54例肺切除术。排除行血管造影及栓塞治疗者。具备以下情况时行手术治疗:1)复发性曲菌球相关咯血;2)明确的单纯性或复杂性曲菌球;3)双侧同时存在曲菌球。
复杂性曲菌球患者吸烟量大、体重指数较低,肺功能参数降低。主要症状为反复咯血、慢性咳嗽、大量脓性痰及呼吸道感染。肺叶切除术是最常采用的术式。B组楔形切除术数量多于A组,差异有统计学意义(p = 0.001)。术后A组并发症发生率(16%)高于B组(9%),差异有统计学意义(p = 0.026)。中位随访时间为30个月(范围19 - 52个月)。胸腔闭式引流管中位留置时间为4天。A组胸腔闭式引流管留置时间更长(4.7±1.4对2.9±1.3;p = 0.005)。A组术后持续性漏气更常见(14.75%;对1.8%,p = 0.015)。A组3例、B组2例因术后血胸行二次手术。支气管胸膜瘘仅发生于A组(n = 4)。
手术切除应采用多学科方法。术前介入治疗可优化手术条件。对于局限性致病病变,手术完全切除必须是首选治疗方法。