Janković Janko, Erić Miloš, Stojisavljević Dragana, Marinković Jelena, Janković Slavenka
Institute of Social Medicine, Faculty of Medicine, University of Belgrade, Belgrade, Serbia.
Center for European Integration and Public Management, Faculty of Economics, Finance and Administration, Singidunum University, Belgrade, Serbia.
PLoS One. 2015 Oct 29;10(10):e0141731. doi: 10.1371/journal.pone.0141731. eCollection 2015.
A relatively consistent body of literature, mainly from high-income countries, supports an inverse association between socio-economic status (SES) and risk of cardiovascular disease (CVD). Data from low- and middle-income countries are scarce. This study explores SES differences in cardiovascular health (CVH) in the Republic of Srpska (RS), Bosnia and Herzegovina, a middle-income country.
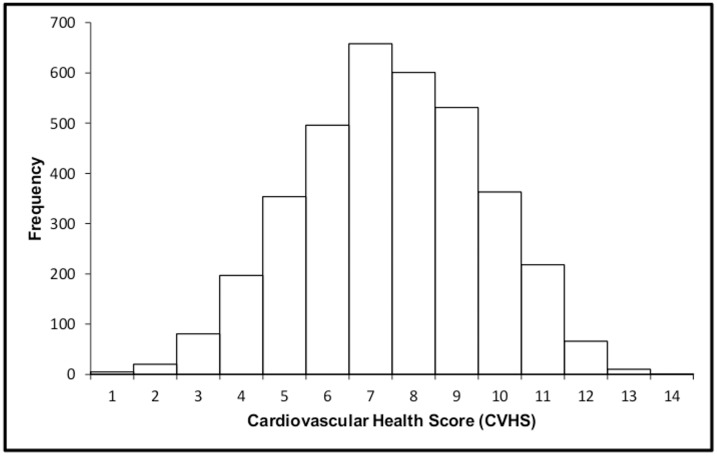
We collected information on SES (education, employment status and household's relative economic status, i.e. household wealth) and the 7 ideal CVH components (smoking status, body mass index, physical activity, diet, blood pressure, total cholesterol, and fasting blood glucose) among 3601 participants 25 years of age and older, from the 2010 National Health Survey in the RS. Based on the sum of all 7 CVH components an overall CVH score (CVHS) was calculated ranging from 0 (all CVH components at poor levels) to 14 (all CVH components at ideal levels). To assess the differences between groups the chi-square test, t-test and ANOVA were used where appropriate. The association between SES and CVHS was analysed with multivariate linear regression analyses. The dependent variable was CVHS, while independent variables were educational level, employment status and wealth index.
According to multiple linear regression analysis CVHS was independently associated with education attainment and employment status. Participants with higher educational attainment and those economically active had higher CVHS (b = 0.57; CI = 0.29-0.85 and b = 0.27; CI = 0.10-0.44 respectively) after adjustment for sex, age group, type of settlement, and marital status. We failed to find any statistically significant difference between the wealth index and CVHS.
This study presents the novel information, since CVHS generated from the individual CVH components was not compared by socio-economic status till now. Our finding that the higher overall CVHS was independently associated with a higher education attainment and those economically active supports the importance of reducing socio-economic inequalities in CVH in RS.
主要来自高收入国家的相对一致的文献资料支持社会经济地位(SES)与心血管疾病(CVD)风险之间存在负相关关系。来自低收入和中等收入国家的数据很少。本研究探讨了波斯尼亚和黑塞哥维那斯普斯卡共和国(RS)这一中等收入国家心血管健康(CVH)方面的社会经济地位差异。
我们收集了2010年RS全国健康调查中3601名25岁及以上参与者的社会经济地位信息(教育程度、就业状况和家庭相对经济状况,即家庭财富)以及7个理想的心血管健康组成部分(吸烟状况、体重指数、身体活动、饮食、血压、总胆固醇和空腹血糖)。根据所有7个心血管健康组成部分的总和计算出一个总体心血管健康评分(CVHS),范围从0(所有心血管健康组成部分处于较差水平)到14(所有心血管健康组成部分处于理想水平)。为评估组间差异,在适当情况下使用了卡方检验、t检验和方差分析。通过多元线性回归分析来分析社会经济地位与CVHS之间的关联。因变量是CVHS,自变量是教育水平、就业状况和财富指数。
根据多元线性回归分析,CVHS与教育程度和就业状况独立相关。在对性别、年龄组、居住地类型和婚姻状况进行调整后,教育程度较高的参与者和经济活跃的参与者的CVHS更高(分别为b = 0.57;CI = 0.29 - 0.85和b = 0.27;CI = 0.10 - 0.44)。我们未发现财富指数与CVHS之间存在任何统计学上的显著差异。
本研究提供了新的信息,因为到目前为止,尚未按社会经济地位对由各个心血管健康组成部分生成的CVHS进行比较。我们的研究结果表明,较高的总体CVHS与较高的教育程度以及经济活跃的人群独立相关,这支持了减少RS心血管健康方面社会经济不平等的重要性。