Mathew Joseph L, Singhi Sunit, Ray Pallab, Hagel Eva, Saghafian-Hedengren Shanie, Bansal Arun, Ygberg Sofia, Sodhi Kushaljit Singh, Kumar B V Ravi, Nilsson Anna
Department of Pediatrics, PGIMER, Chandigarh, India.
Department of Medical Microbiology, PGIMER, Chandigarh, India.
J Glob Health. 2015 Dec;5(2):050418. doi: 10.7189/jogh.05.020418.
Childhood community acquired pneumonia (CAP) is a significant problem in developing countries, and confirmation of microbial etiology is important for individual, as well as public health. However, there is paucity of data from a large cohort, examining multiple biological specimens for diverse pathogens (bacteria and viruses). The Community Acquired Pneumonia Etiology Study (CAPES) was designed to address this knowledge gap.
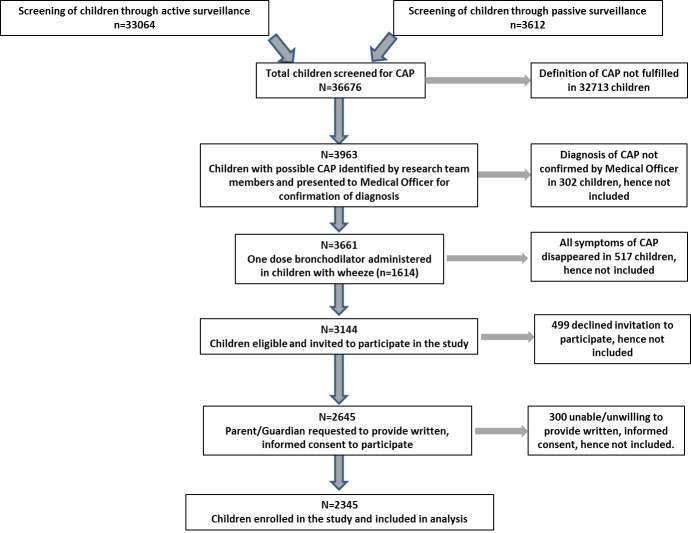
We enrolled children with CAP (based on WHO IMCI criteria of tachypnea with cough or breathing difficulty) over 24 consecutive months, and recorded presenting symptoms, risk factors, clinical signs, and chest radiography. We performed blood and nasopharyngeal aspirate (NPA) bacterial cultures, and serology (Mycoplasma pneumoniae, Chlamydophila pneumoniae). We also performed multiplex PCR for 25 bacterial/viral species in a subgroup representing 20% of the cohort. Children requiring endotracheal intubation underwent culture and PCR of bronchoalveolar lavage (BAL) specimens.
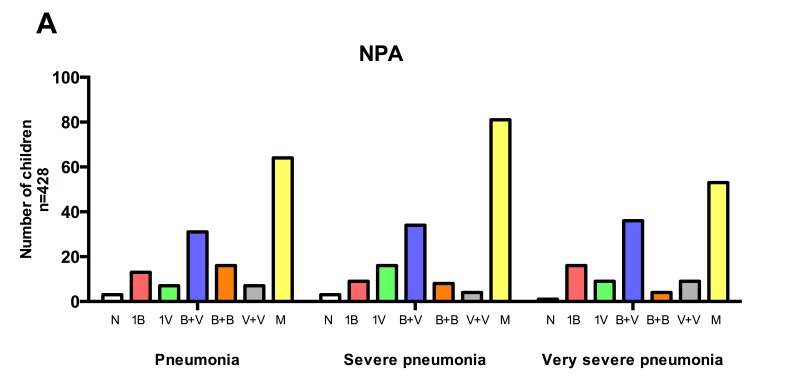
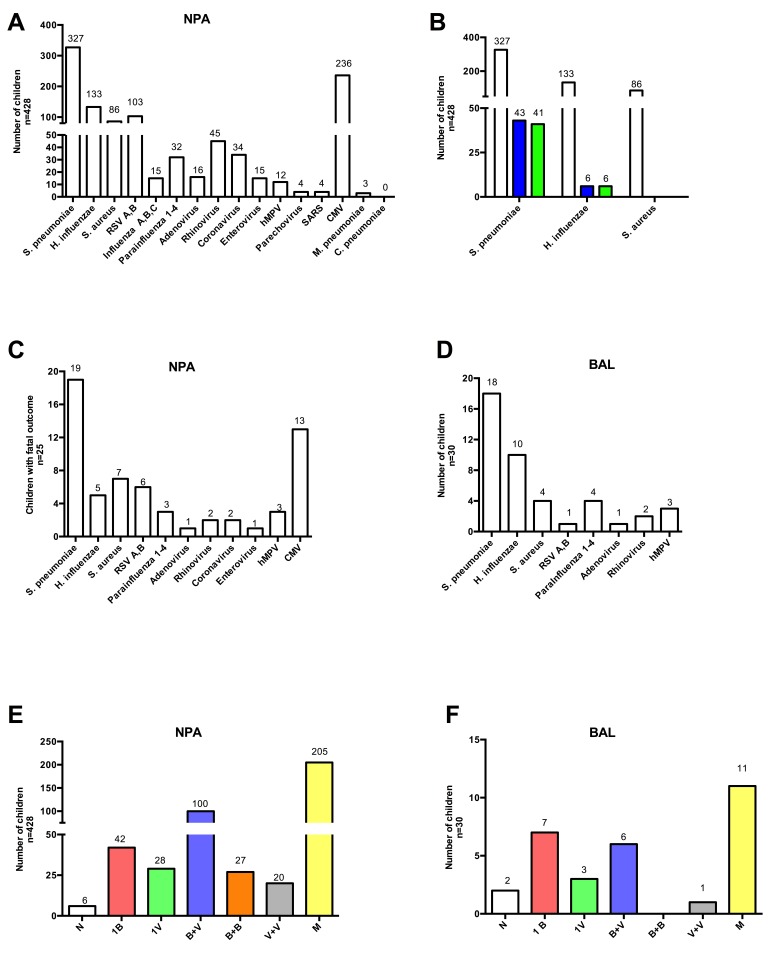
We enrolled 2345 children. NPA and blood cultures yielded bacteria in only 322 (13.7%) and 49 (2.1%) children respectively. In NPA, Streptococcus pneumoniae (79.1%) predominated, followed by Haemophilus influenzae (9.6%) and Staphylococcus aureus (6.8%). In blood, S. aureus (30.6%) dominated, followed by S. pneumoniae (20.4%) and Klebsiella pneumoniae (12.2%). M. pneumoniae and C. pneumoniae serology were positive in 4.3% and 1.1% respectively. Multiplex PCR in 428 NPA specimens identified organisms in 422 (98.6%); of these 352 (82.2%) had multiple organisms and only 70 (16.4%) had a single organism viz. S. pneumoniae: 35 (50%), Cytomegalovirus (CMV): 13 (18.6%), Respiratory Syncytial Virus (RSV): 9 (12.9%), other viruses: 6 (8.7%), S. aureus: 5 (7.1%), and H. influenzae: 2 (2.9%). BAL PCR (n = 30) identified single pathogens in 10 (S. pneumoniae-3, CMV-3, S. aureus-2, H. influenzae-2) and multiple pathogens in 18 children. There were 108 (4.6%) deaths. The pattern of pathogens identified did not correlate with pneumonia severity or mortality.
The majority of children with CAP have multiple pathogens (bacteria and viruses). S. pneumoniae and S. aureus predominate in NPA and blood respectively. CMV and RSV were the dominant respiratory viruses in NPA and BAL. The presence of multiple pathogens, especially organisms associated with nasopharyngeal carriage, precludes confirmation of a causal relationship in most cases.
儿童社区获得性肺炎(CAP)在发展中国家是一个重大问题,微生物病因的确诊对个体健康以及公共卫生都很重要。然而,来自大型队列研究、针对多种病原体(细菌和病毒)检测多个生物标本的数据匮乏。社区获得性肺炎病因学研究(CAPES)旨在填补这一知识空白。
我们连续24个月纳入符合CAP标准(基于世界卫生组织IMCI标准,即呼吸急促伴咳嗽或呼吸困难)的儿童,记录其就诊症状、危险因素、临床体征及胸部X线检查结果。我们进行了血液和鼻咽抽吸物(NPA)细菌培养以及血清学检测(肺炎支原体、肺炎衣原体)。我们还对占队列20%的一个亚组中的25种细菌/病毒进行了多重PCR检测。需要气管插管的儿童接受支气管肺泡灌洗(BAL)标本培养和PCR检测。
我们共纳入2345名儿童。NPA和血液培养分别仅在322名(13.7%)和49名(2.1%)儿童中培养出细菌。在NPA中,肺炎链球菌(79.1%)占主导,其次是流感嗜血杆菌(9.6%)和金黄色葡萄球菌(6.8%)。在血液中,金黄色葡萄球菌(30.6%)占主导,其次是肺炎链球菌(20.4%)和肺炎克雷伯菌(12.2%)。肺炎支原体和肺炎衣原体血清学检测阳性率分别为4.3%和1.1%。对428份NPA标本进行的多重PCR检测在422份(98.6%)标本中鉴定出病原体;其中352份(82.2%)有多种病原体,仅70份(16.4%)有单一病原体,即肺炎链球菌:35份(50%)、巨细胞病毒(CMV):13份(18.6%)、呼吸道合胞病毒(RSV):9份(12.9%)、其他病毒:6份(8.7%)、金黄色葡萄球菌:5份(7.1%)、流感嗜血杆菌:2份(2.9%)。BAL PCR(n = 30)在10名儿童中鉴定出单一病原体(肺炎链球菌 - 3例、CMV - 3例、金黄色葡萄球菌 - 2例、流感嗜血杆菌 - 2例),在18名儿童中鉴定出多种病原体。共有108例(4.6%)死亡。所鉴定的病原体模式与肺炎严重程度或死亡率无关。
大多数CAP儿童有多种病原体(细菌和病毒)。肺炎链球菌和金黄色葡萄球菌分别在NPA和血液中占主导。CMV和RSV是NPA和BAL中主要的呼吸道病毒。多种病原体的存在,尤其是与鼻咽部携带相关的病原体,使得在大多数情况下难以确定因果关系。