Gifford Katherine A, Liu Dandan, Hohman Timothy J, Xu Meng, Han Xue, Romano Raymond R, Fritzsche Laura R, Abel Ty, Jefferson Angela L
Vanderbilt Memory & Alzheimer's Center, Department of Neurology, Vanderbilt University Medical Center, Nashville, Tennessee, United States of America.
Department of Biostatistics, Vanderbilt University School of Medicine, Nashville, Tennessee, United States of America.
PLoS One. 2015 Nov 5;10(11):e0141831. doi: 10.1371/journal.pone.0141831. eCollection 2015.
This study examines whether different sources of cognitive complaint (i.e., self and informant) predict Alzheimer's disease (AD) neuropathology in elders with mild cognitive impairment (MCI).
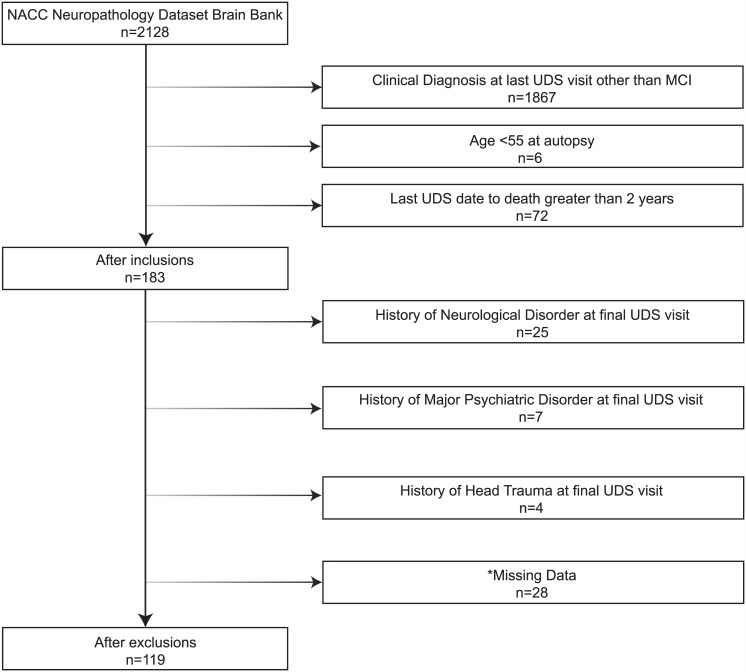
Data were drawn from the National Alzheimer's Coordinating Center Uniform and Neuropathology Datasets (observational studies) for participants with a clinical diagnosis of MCI and postmortem examination (n = 1843, 74±8 years, 52% female). Cognitive complaint (0.9±0.5 years prior to autopsy) was classified into four mutually exclusive groups: no complaint, self-only, informant-only, or mutual (both self and informant) complaint. Postmortem neuropathological outcomes included amyloid plaques and neurofibrillary tangles. Proportional odds regression related complaint to neuropathology, adjusting for age, sex, race, education, depressed mood, cognition, APOE4 status, and last clinical visit to death interval.
Mutual complaint related to increased likelihood of meeting NIA/Reagan Institute (OR = 6.58, p = 0.004) and Consortium to Establish a Registry for Alzheimer's Disease criteria (OR = 5.82, p = 0.03), and increased neurofibrillary tangles (OR = 3.70, p = 0.03), neuritic plaques (OR = 3.52, p = 0.03), and diffuse plaques (OR = 4.35, p = 0.02). Informant-only and self-only complaint was not associated with any neuropathological outcome (all p-values>0.12).
In MCI, mutual cognitive complaint relates to AD pathology whereas self-only or informant-only complaint shows no relation to pathology. Findings support cognitive complaint as a marker of unhealthy brain aging and highlight the importance of obtaining informant corroboration to increase confidence of underlying pathological processes.
本研究探讨不同认知主诉来源(即自我报告和他人报告)是否能预测轻度认知障碍(MCI)老年人的阿尔茨海默病(AD)神经病理学特征。
数据来自国家阿尔茨海默病协调中心统一数据集和神经病理学数据集(观察性研究),研究对象为临床诊断为MCI且接受过尸检的参与者(n = 1843,年龄74±8岁,女性占52%)。认知主诉(尸检前0.9±0.5年)分为四个相互排斥的组:无主诉、仅自我报告、仅他人报告或共同主诉(自我报告和他人报告均有)。尸检后的神经病理学结果包括淀粉样斑块和神经原纤维缠结。采用比例优势回归分析主诉与神经病理学之间的关系,并对年龄、性别、种族、教育程度、抑郁情绪、认知、APOE4状态以及最后一次临床就诊至死亡间隔进行校正。
共同主诉与符合美国国立衰老研究所/里根研究所标准(比值比[OR]=6.58,p = 0.004)和阿尔茨海默病注册协会标准(OR = 5.82,p = 0.03)的可能性增加相关,并且神经原纤维缠结(OR = 3.70,p = 0.03)、神经炎斑块(OR = 3.52,p = 0.03)和弥漫性斑块(OR = 4.35,p = 0.02)增多。仅他人报告和仅自我报告的主诉与任何神经病理学结果均无关联(所有p值>0.12)。
在MCI中,共同认知主诉与AD病理学相关,而仅自我报告或仅他人报告的主诉与病理学无关。研究结果支持将认知主诉作为不健康脑老化的标志物,并强调获取他人佐证以提高对潜在病理过程信心的重要性。