Suarez Jonathan J, Isakova Tamara, Anderson Cheryl A M, Boulware L Ebony, Wolf Myles, Scialla Julia J
Department of Medicine, University of Miami Miller School of Medicine, Miami, Florida; Department of Medicine, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania.
Department of Medicine, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Am J Prev Med. 2015 Dec;49(6):912-20. doi: 10.1016/j.amepre.2015.07.017.
Greater distance to full-service supermarkets and low income may impair access to healthy diets and contribute to chronic kidney disease (CKD) and hypertension. The study aim was to determine relationships among residence in a "food desert," low income, CKD, and blood pressure.
Adults in the 2003-2010 National Health and Nutrition Examination Survey (N=22,173) were linked to food desert data (www.ers.usda.gov) by Census Tracts. Food deserts have low median income and are further from a supermarket or large grocery store (>1 mile in urban areas, >10 miles in rural areas). Weighted regression was used to determine the association of residence in a food desert and family income with dietary intake; systolic blood pressure (SBP); and odds of CKD. Data analysis was performed in 2014-2015.
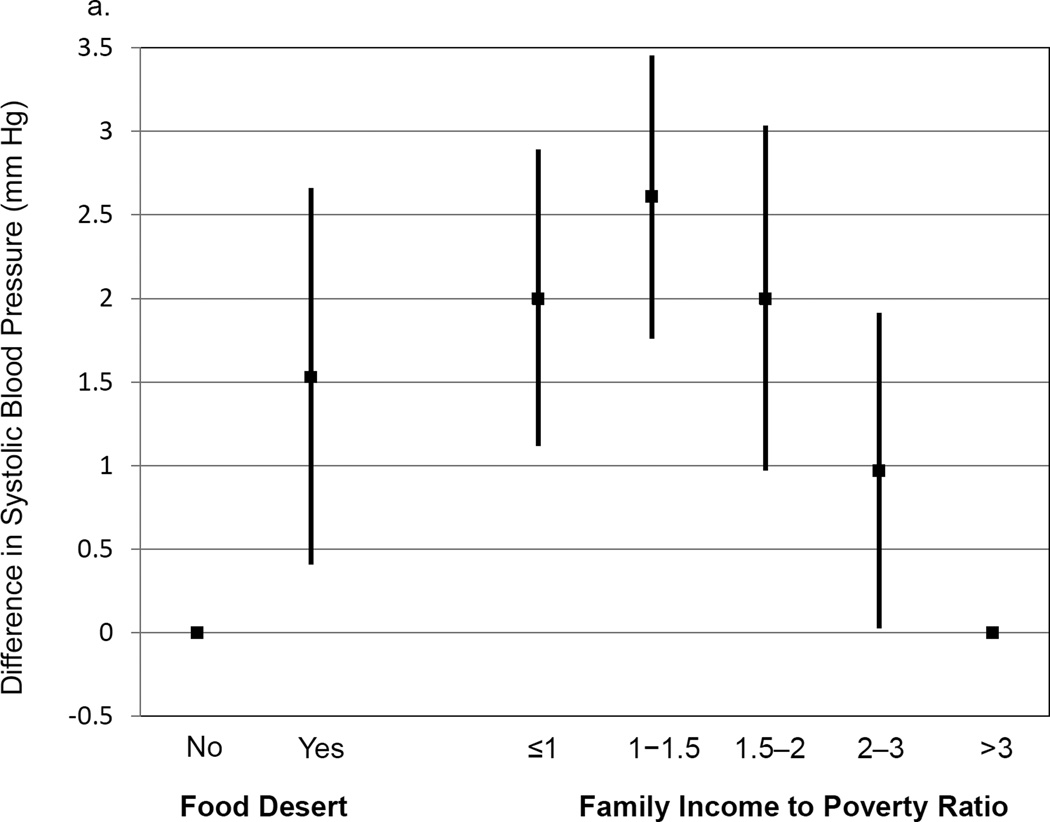
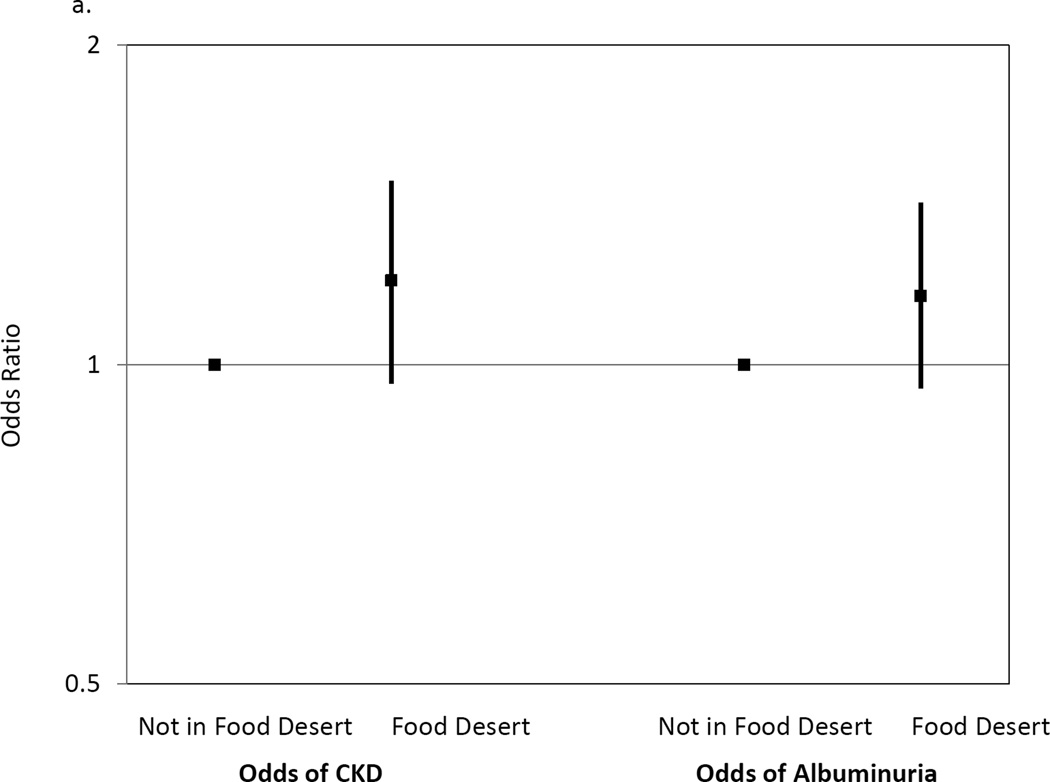
Compared with those not in food deserts, participants residing in food deserts had lower levels of serum carotenoids (p<0.01), a biomarker of fruit and vegetable intake, and higher SBP (1.53 mmHg higher, 95% CI=0.41, 2.66) after adjustment for demographics and income. Residence in a food desert was not associated with odds of CKD (OR=1.20, 95% CI=0.96, 1.49). Lower, versus higher, income was associated with lower serum carotenoids (p<0.01) and higher SBP (2.00 mmHg higher for income-poverty ratio ≤1 vs >3, 95% CI=1.12, 2.89), but also greater odds of CKD (OR=1.76 for income-poverty ratio ≤1 vs >3, 95% CI=1.48, 2.10).
Limited access to healthy food due to geographic or financial barriers could be targeted for prevention of CKD and hypertension.
距离提供全方位服务的超市较远以及低收入可能会影响获得健康饮食的机会,并导致慢性肾脏病(CKD)和高血压。本研究的目的是确定居住在“食物荒漠”、低收入、CKD和血压之间的关系。
通过人口普查区将2003 - 2010年美国国家健康与营养检查调查中的成年人(N = 22173)与食物荒漠数据(www.ers.usda.gov)相关联。食物荒漠的收入中位数较低,且距离超市或大型杂货店较远(城市地区大于1英里,农村地区大于10英里)。采用加权回归来确定居住在食物荒漠和家庭收入与饮食摄入量、收缩压(SBP)以及CKD患病几率之间的关联。数据分析于2014 - 2015年进行。
与不住在食物荒漠地区的参与者相比,居住在食物荒漠地区的参与者血清类胡萝卜素水平较低(p<0.01),血清类胡萝卜素是水果和蔬菜摄入量的生物标志物,在对人口统计学和收入进行调整后,收缩压较高(高1.53 mmHg,95%置信区间=0.41, 2.66)。居住在食物荒漠地区与CKD患病几率无关(比值比=1.20,95%置信区间=0.96, 1.49)。与高收入相比,低收入与较低的血清类胡萝卜素水平(p<0.01)和较高的收缩压相关(收入贫困比≤1时比>3时高2.00 mmHg,95%置信区间=1.12, 2.89),但CKD患病几率也更高(收入贫困比≤1时比>3时的比值比=1.76,95%置信区间=1.48, 2.10)。
由于地理或经济障碍导致获得健康食物的机会有限,这可能是预防CKD和高血压的目标。