Ito Fumito, Ku Amy W, Bucsek Mark J, Muhitch Jason B, Vardam-Kaur Trupti, Kim Minhyung, Fisher Daniel T, Camoriano Marta, Khoury Thaer, Skitzki Joseph J, Gollnick Sandra O, Evans Sharon S
Department of Immunology, Roswell Park Cancer Institute, Buffalo, New York, United States of America.
Department of Surgical Oncology, Roswell Park Cancer Institute, Buffalo, New York, United States of America.
PLoS One. 2015 Nov 23;10(11):e0143370. doi: 10.1371/journal.pone.0143370. eCollection 2015.
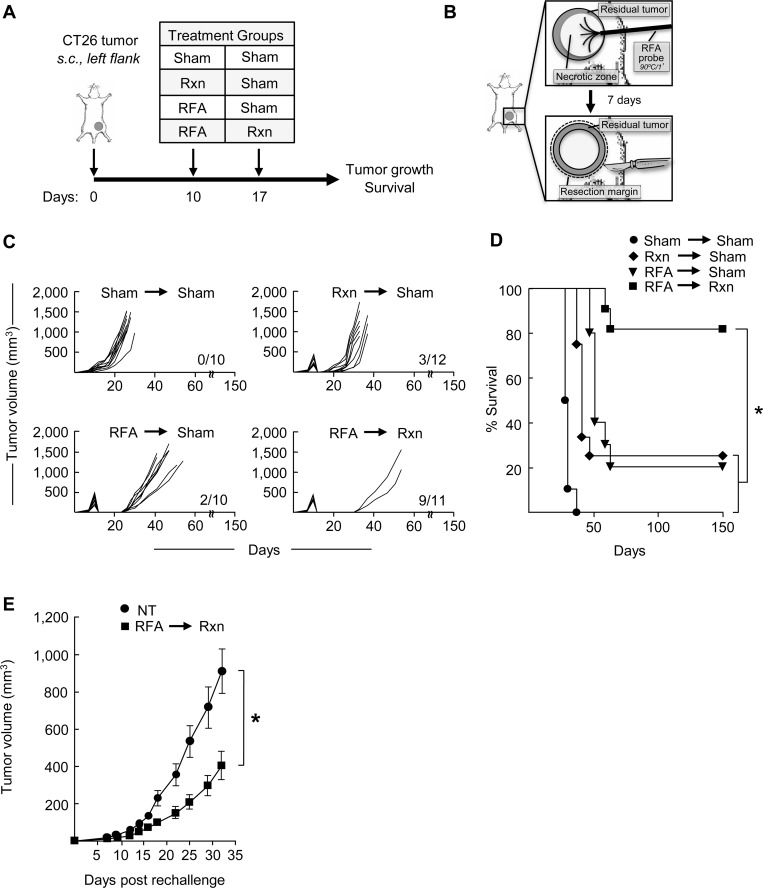
While surgical resection is a cornerstone of cancer treatment, local and distant recurrences continue to adversely affect outcome in a significant proportion of patients. Evidence that an alternative debulking strategy involving radiofrequency ablation (RFA) induces antitumor immunity prompted the current investigation of the efficacy of performing RFA prior to surgical resection (pre-resectional RFA) in a preclinical mouse model.
Therapeutic efficacy and systemic immune responses were assessed following pre-resectional RFA treatment of murine CT26 colon adenocarcinoma.
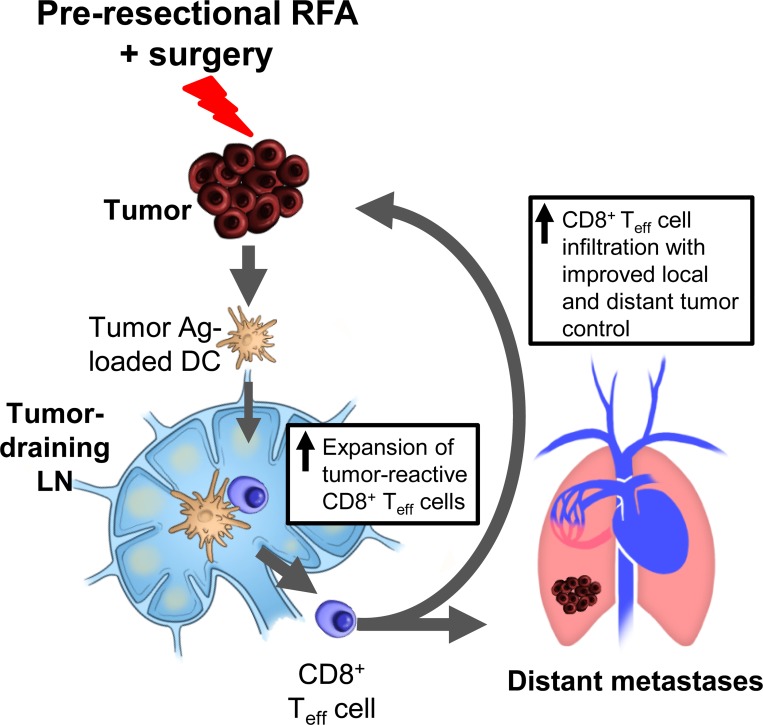
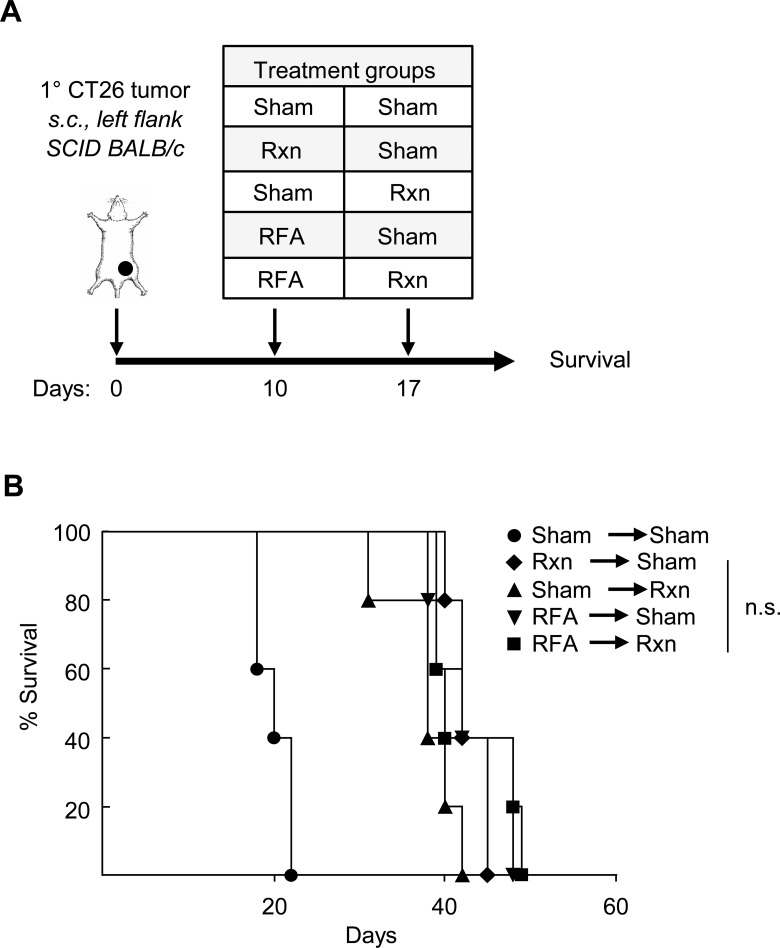
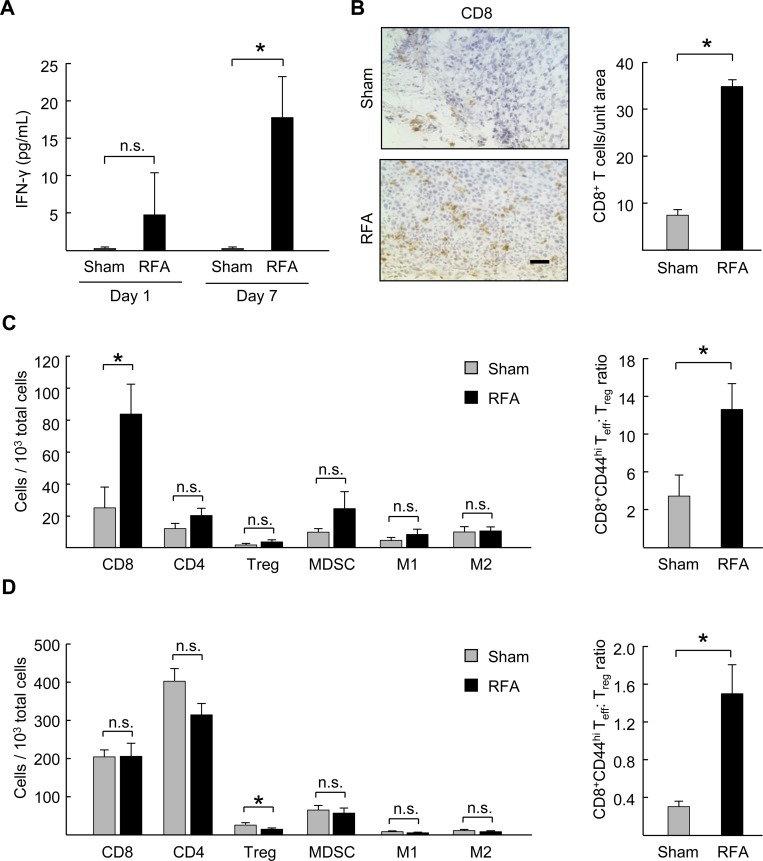
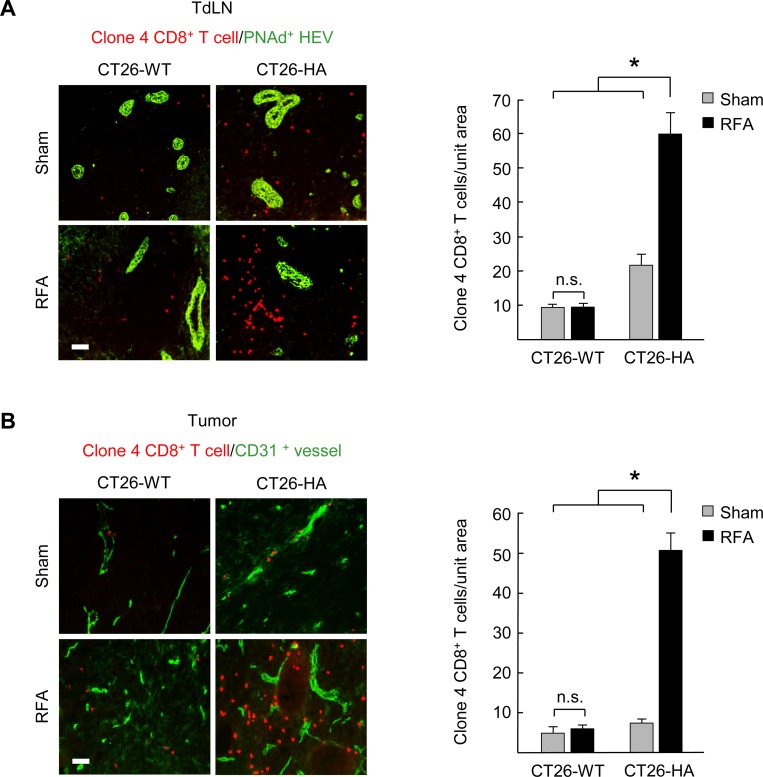
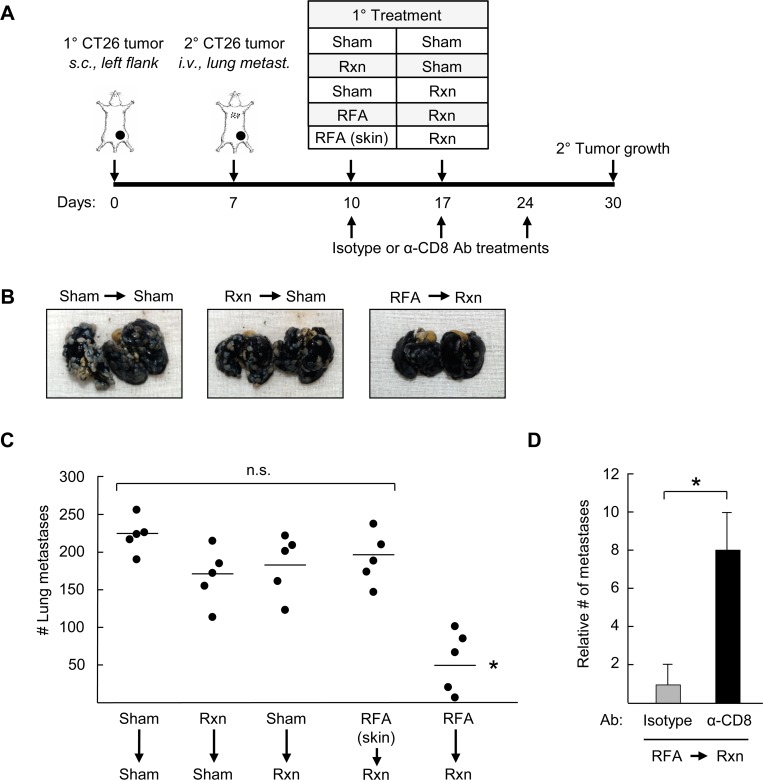
Treatment with pre-resectional RFA significantly delayed tumor growth and improved overall survival compared to sham surgery, RFA, or resection alone. Mice in the pre-resectional RFA group that achieved a complete response demonstrated durable antitumor immunity upon tumor re-challenge. Failure to achieve a therapeutic benefit in immunodeficient mice confirmed that tumor control by pre-resectional RFA depends on an intact adaptive immune response rather than changes in physical parameters that make ablated tumors more amenable to a complete surgical excision. RFA causes a marked increase in intratumoral CD8+ T lymphocyte infiltration, thus substantially enhancing the ratio of CD8+ effector T cells: FoxP3+ regulatory T cells. Importantly, pre-resectional RFA significantly increases the number of antigen-specific CD8+ T cells within the tumor microenvironment and tumor-draining lymph node but had no impact on infiltration by myeloid-derived suppressor cells, M1 macrophages or M2 macrophages at tumor sites or in peripheral lymphoid organs (i.e., spleen). Finally, pre-resectional RFA of primary tumors delayed growth of distant tumors through a mechanism that depends on systemic CD8+ T cell-mediated antitumor immunity.
Improved survival and antitumor systemic immunity elicited by pre-resectional RFA support the translational potential of this neoadjuvant treatment for cancer patients with high-risk of local and systemic recurrence.
虽然手术切除是癌症治疗的基石,但局部和远处复发仍会对相当一部分患者的治疗结果产生不利影响。有证据表明,一种涉及射频消融(RFA)的替代减瘤策略可诱导抗肿瘤免疫,这促使我们在临床前小鼠模型中对手术切除前进行RFA(切除前RFA)的疗效进行了当前研究。
对小鼠CT26结肠腺癌进行切除前RFA治疗后,评估其治疗效果和全身免疫反应。
与假手术、单纯RFA或单纯切除相比,切除前RFA治疗显著延迟了肿瘤生长并提高了总生存率。切除前RFA组中达到完全缓解的小鼠在肿瘤再次激发时表现出持久的抗肿瘤免疫。免疫缺陷小鼠未获得治疗益处,这证实切除前RFA对肿瘤的控制依赖于完整的适应性免疫反应,而非使消融肿瘤更易于完全手术切除的物理参数变化。RFA导致肿瘤内CD8 + T淋巴细胞浸润显著增加,从而大幅提高了CD8 +效应T细胞与FoxP3 +调节性T细胞的比例。重要的是,切除前RFA显著增加了肿瘤微环境和肿瘤引流淋巴结内抗原特异性CD8 + T细胞的数量,但对肿瘤部位或外周淋巴器官(即脾脏)中髓源性抑制细胞、M1巨噬细胞或M2巨噬细胞的浸润没有影响。最后,原发性肿瘤的切除前RFA通过一种依赖于全身CD8 + T细胞介导的抗肿瘤免疫的机制延迟了远处肿瘤的生长。
切除前RFA所带来的生存率提高和抗肿瘤全身免疫支持了这种新辅助治疗对于局部和全身复发高风险癌症患者的转化潜力。