Shi Liangrong, Chen Lujun, Wu Changping, Zhu Yibei, Xu Bin, Zheng Xiao, Sun Mingfen, Wen Wen, Dai Xichao, Yang Min, Lv Quansheng, Lu Binfeng, Jiang Jingting
Department of Tumor Biological Treatment, Soochow University, Changzhou 213003, Jiangsu, China.
Department of Oncology, the Third Affiliated Hospital, Soochow University, Changzhou 213003, Jiangsu, China.
Clin Cancer Res. 2016 Mar 1;22(5):1173-1184. doi: 10.1158/1078-0432.CCR-15-1352.
Radiofrequency ablation (RFA) has been shown to elicit tumor-specific T-cell immune responses, but is not sufficient to prevent cancer progression. Here, we investigated immune-suppressive mechanisms limiting the efficacy of RFA.
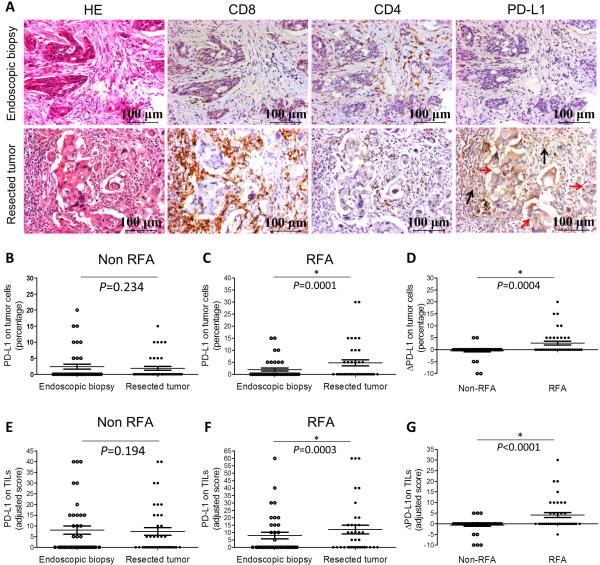
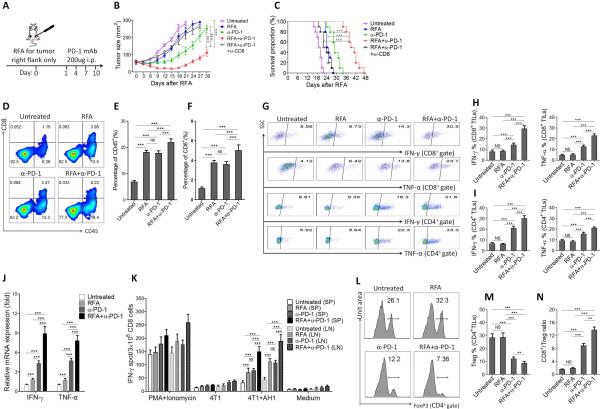
We performed a retrospective case-controlled study on patients with synchronous colorectal cancer liver metastases who had received primary tumor resection with or without preoperative RFA for liver metastases. Tumor-infiltrating T cells and tumoral PD-L1 expression in human colorectal cancer tissues were analyzed by immunohistochemistry. T-cell immune responses and PD-1/PD-L1 expression were also characterized in an RFA mouse model. In addition, the combined effect of RAF and PD-1 blockade was evaluated in the mouse RFA model.
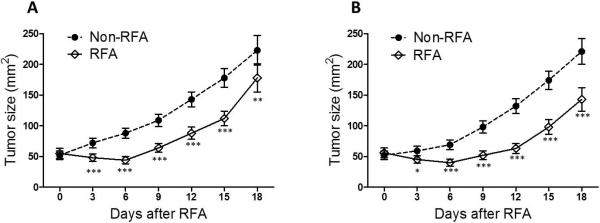
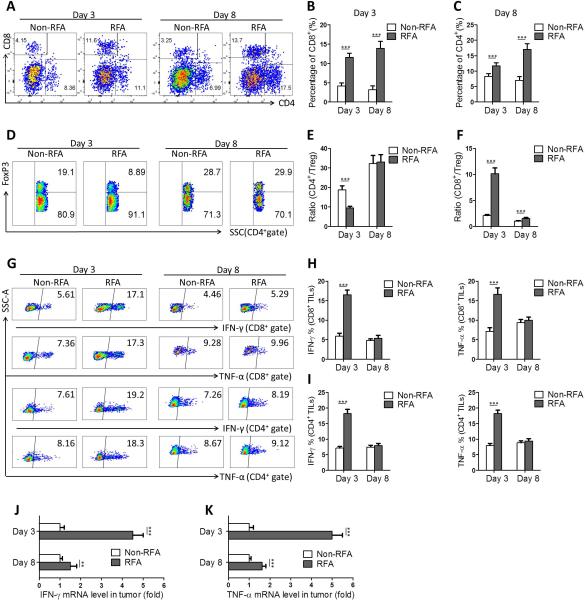
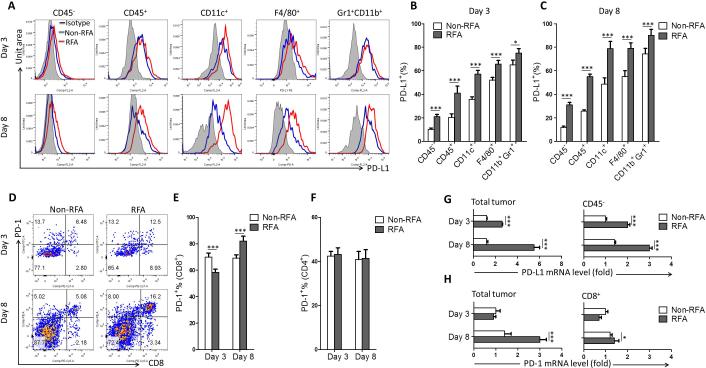
We found that RFA treatment of liver metastases increased not only T-cell infiltration, but also PD-L1 expression in primary human colorectal tumors. Using mouse tumor models, we demonstrated that RFA treatment of one tumor initially enhanced a strong T-cell-mediated immune response in tumor. Nevertheless, tumor quickly overcame the immune responses by inhibiting the function of CD8(+) and CD4(+) T cells, driving a shift to higher regulatory T-cell to Teff ratio, and upregulating PD-L1/PD-1 expression. Furthermore, we established that the combined therapy of RFA and anti-PD-1 antibodies significantly enhanced T-cell immune responses, resulting in stronger antitumor immunity and prolonged survival.
The PD-L1-PD-1 axis plays a critical role in dampening RFA-induced antitumor immune responses, and this study provides a strong rationale for combining RFA and the PD-L1/PD-1 blockade in the clinical setting.
射频消融(RFA)已被证明可引发肿瘤特异性T细胞免疫反应,但不足以预防癌症进展。在此,我们研究了限制RFA疗效的免疫抑制机制。
我们对患有同步性结直肠癌肝转移且接受了肝转移瘤术前RFA或未接受术前RFA的原发肿瘤切除术的患者进行了一项回顾性病例对照研究。通过免疫组织化学分析人结直肠癌组织中的肿瘤浸润T细胞和肿瘤PD-L1表达。在RFA小鼠模型中也对T细胞免疫反应和PD-1/PD-L1表达进行了表征。此外,在小鼠RFA模型中评估了RFA与PD-1阻断的联合作用。
我们发现对肝转移瘤进行RFA治疗不仅增加了T细胞浸润,还增加了原发性人结直肠癌肿瘤中的PD-L1表达。使用小鼠肿瘤模型,我们证明对一个肿瘤进行RFA治疗最初会增强肿瘤中强烈的T细胞介导的免疫反应。然而,肿瘤通过抑制CD8(+)和CD4(+) T细胞的功能、促使调节性T细胞与效应T细胞的比例升高以及上调PD-L1/PD-1表达,迅速克服了免疫反应。此外,我们证实RFA与抗PD-1抗体的联合治疗显著增强了T细胞免疫反应,从而产生更强的抗肿瘤免疫力并延长了生存期。
PD-L1-PD-1轴在减弱RFA诱导的抗肿瘤免疫反应中起关键作用,并且本研究为在临床环境中联合使用RFA与PD-L1/PD-1阻断提供了有力的理论依据。