Sagara Issaka, Beavogui Abdoul Habib, Zongo Issaka, Soulama Issiaka, Borghini-Fuhrer Isabelle, Fofana Bakary, Camara Daouda, Somé Anyirékun F, Coulibaly Aboubacar S, Traore Oumar B, Dara Niawanlou, Kabore Moïse J T, Thera Ismaila, Compaore Yves D, Sylla Malick Minkael, Nikiema Frederic, Diallo Mamadou Saliou, Dicko Alassane, Gil Jose Pedro, Borrmann Steffen, Duparc Stephan, Miller Robert M, Doumbo Ogobara K, Shin Jangsik, Bjorkman Anders, Ouedraogo Jean-Bosco, Sirima Sodiomon B, Djimdé Abdoulaye A
Malaria Research and Training Center, Department of Epidemiology of Parasitic Diseases, Faculty of Pharmacy, University of Science, Techniques and Technologies of Bamako, Mali.
Centre de Formation et de Recherche en Santé Rurale de Mafèrinyah, Conakry, Guinea.
Lancet Infect Dis. 2016 Feb;16(2):189-98. doi: 10.1016/S1473-3099(15)00318-7. Epub 2015 Oct 23.
Sparse data on the safety of pyronaridine-artesunate after repeated treatment of malaria episodes restrict its clinical use. We therefore compared the safety of pyronaridine-artesunate after treatment of the first episode of malaria versus re-treatment in a substudy analysis.
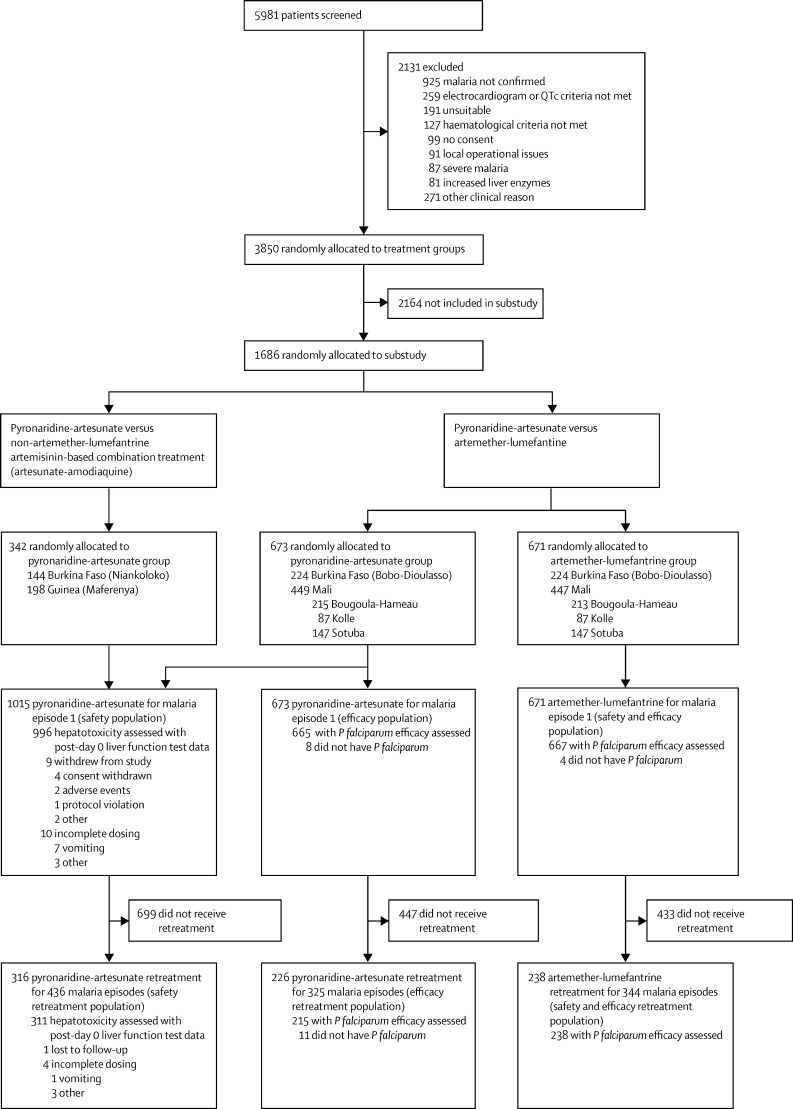
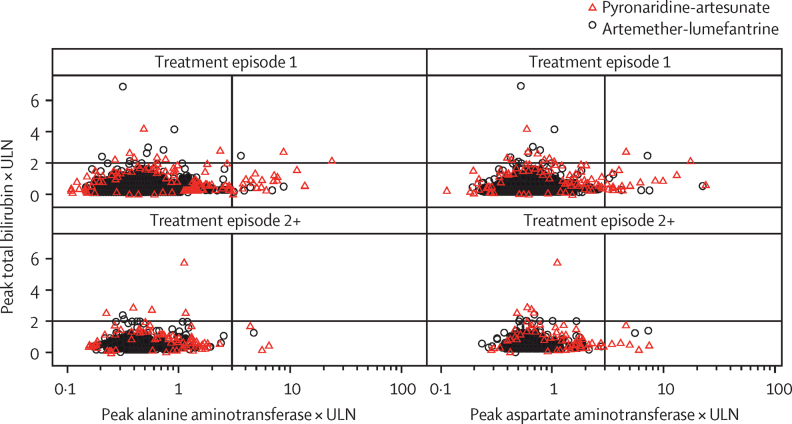
This planned substudy analysis of the randomised, open-label West African Network for Clinical Trials of Antimalarial Drugs (WANECAM) phase 3b/4 trial was done at six health facilities in Mali, Burkina Faso, and Guinea in patients (aged ≥6 months and bodyweight ≥5 kg) with uncomplicated microscopically confirmed Plasmodium spp malaria (parasite density <200 000 per μL blood) and fever or history of fever. The primary safety endpoint was incidence of hepatotoxicity: alanine aminotransferase of greater than five times the upper limit of normal (ULN) or Hy's criteria (alanine aminotransferase or aspartate aminotransferase greater than three times the ULN and total bilirubin more than twice the ULN) after treatment of the first episode of malaria and re-treatment (≥28 days after first treatment) with pyronaridine-artesunate. Pyronaridine-artesunate efficacy was compared with artemether-lumefantrine with the adequate clinical and parasitological response (ACPR) in an intention-to-treat analysis. WANECAM is registered with PACTR.org, number PACTR201105000286876.
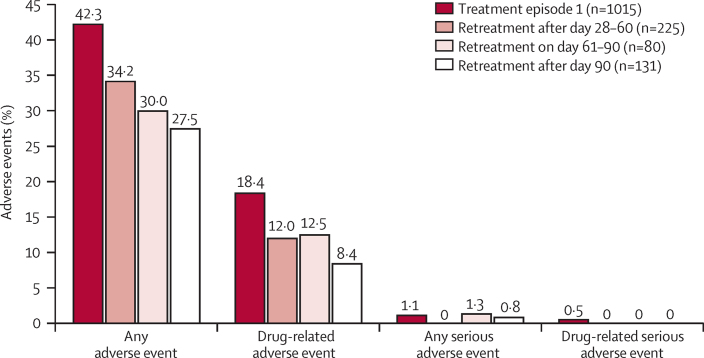
Following first treatment, 13 (1%) of 996 patients had hepatotoxicity (including one [<1%] possible Hy's law case) versus two (1%) of 311 patients on re-treatment (neither a Hy's law case). No evidence was found that pyronaridine-artesunate re-treatment increased safety risk based on laboratory values, reported adverse event frequencies, or electrocardiograph findings. For all first treatment or re-treatment episodes, pyronaridine-artesunate (n=673) day 28 crude ACPR was 92·7% (95% CI 91·0-94·3) versus 80·4% (77·8-83·0) for artemether-lumefantrine (n=671). After exclusion of patients with PCR-confirmed new infections, ACPR was similar on treatment and re-treatment and greater than 95% at day 28 and greater than 91% at day 42 in both treatment groups.
The findings that pyronaridine-artesunate safety and efficacy were similar on first malaria treatment versus re-treatment of subsequent episodes lend support for the wider access to pyronaridine-artesunate as an alternative artemisinin-based combination treatment for malaria in sub-Saharan Africa.
European and Developing Countries Clinical Trial Partnership, Medicines for Malaria Venture (Geneva, Switzerland), UK Medical Research Council, Swedish International Development Cooperation Agency, German Ministry for Education and Research, University Claude Bernard (Lyon, France), Malaria Research and Training Centre (Bamako, Mali), Centre National de Recherche et de Formation sur le Paludisme (Burkina Faso), Institut de Recherche en Sciences de la Santé (Bobo-Dioulasso, Burkina Faso), and Centre National de Formation et de Recherche en Santé Rurale (Republic of Guinea).
疟疾发作多次治疗后,咯萘啶 - 青蒿琥酯安全性的数据稀少,限制了其临床应用。因此,我们在一项子研究分析中比较了疟疾首次发作治疗后与再次治疗后咯萘啶 - 青蒿琥酯的安全性。
这项针对抗疟药物西非临床试验网络(WANECAM)3b/4期随机、开放标签试验的计划子研究分析,在马里、布基纳法索和几内亚的六个卫生机构对年龄≥6个月且体重≥5 kg、经显微镜确诊为单纯性疟原虫属疟疾(寄生虫密度<每微升血液200000个)且有发热或发热史的患者进行。主要安全终点是肝毒性的发生率:在首次疟疾发作治疗以及用咯萘啶 - 青蒿琥酯再次治疗(首次治疗后≥28天)后,丙氨酸氨基转移酶大于正常上限(ULN)的五倍或符合Hy氏标准(丙氨酸氨基转移酶或天冬氨酸氨基转移酶大于ULN的三倍且总胆红素超过ULN的两倍)。在一项意向性分析中,将咯萘啶 - 青蒿琥酯的疗效与蒿甲醚 - 本芴醇的充分临床和寄生虫学反应(ACPR)进行比较。WANECAM在PACTR.org注册,注册号为PACTR201105000286876。
首次治疗后,996例患者中有13例(1%)出现肝毒性(包括1例[<1%]可能符合Hy氏法则的病例),而再次治疗的311例患者中有2例(1%)(均不符合Hy氏法则病例)。基于实验室值、报告的不良事件频率或心电图结果,未发现咯萘啶 - 青蒿琥酯再次治疗会增加安全风险的证据。对于所有首次治疗或再次治疗发作,咯萘啶 - 青蒿琥酯(n = 673)第28天的粗ACPR为92.7%(95%CI 91.0 - 94.3),而蒿甲醚 - 本芴醇(n = 671)为80.4%(77.8 - 83.0)。排除PCR确诊有新感染的患者后,两个治疗组在治疗和再次治疗时ACPR相似,第28天大于95%,第42天大于91%。
咯萘啶 - 青蒿琥酯在首次疟疾治疗与后续发作再次治疗时安全性和疗效相似的这一发现,支持更广泛地使用咯萘啶 - 青蒿琥酯作为撒哈拉以南非洲基于青蒿素的疟疾联合治疗的替代药物。
欧洲和发展中国家临床试验合作组织、疟疾药物事业组织(瑞士日内瓦)、英国医学研究理事会、瑞典国际开发合作署、德国教育和研究部、克劳德·伯纳德大学(法国里昂)、疟疾研究与培训中心(马里巴马科)、国家疟疾研究与培训中心(布基纳法索)、健康科学研究所(布基纳法索博博迪乌拉索)以及农村卫生国家培训与研究中心(几内亚共和国)。