Pryce Joseph, Hine Paul
Department of Clinical Sciences, Liverpool School of Tropical Medicine, Pembroke Place, Liverpool, UK, L3 5QA.
Cochrane Database Syst Rev. 2019 Jan 8;1(1):CD006404. doi: 10.1002/14651858.CD006404.pub3.
The World Health Organization (WHO) recommends artemisinin-based combination therapies (ACTs) to treat uncomplicated Plasmodium falciparum (P falciparum) malaria. Concerns about artemisinin resistance have led to global initiatives to develop new partner drugs to protect artemisinin derivatives in ACT. Pyronaridine-artesunate is a novel ACT.
To evaluate the efficacy of pyronaridine-artesunate compared to alternative ACTs for treating people with uncomplicated P falciparum malaria, and to evaluate the safety of pyronaridine-artesunate and other pyronaridine treatments compared to alternative treatments.
We searched the Cochrane Infectious Diseases Group Specialized Register; Cochrane Central Register of Controlled Trials (CENTRAL), published in the Cochrane Library; MEDLINE; Embase; and LILACS. We also searched ClinicalTrials.gov, the WHO International Clinical Trials Registry Platform Search Portal, and the International Standard Randomized Controlled Trial Number (ISRCTN) registry for ongoing or recently completed trials. The date of the last search was 8 May 2018.
Efficacy analysis: randomized controlled trials (RCTs) of pyronaridine-artesunate for treating uncomplicated P falciparum malaria.Safety analysis: RCTs of pyronaridine-artesunate or pyronaridine for treating P falciparum or P vivax malaria.
For this update, two review authors independently re-extracted all data and assessed certainty of evidence. We meta-analysed data to calculate risk ratios (RRs) for treatment failures between comparisons, and for safety outcomes between and across comparisons.
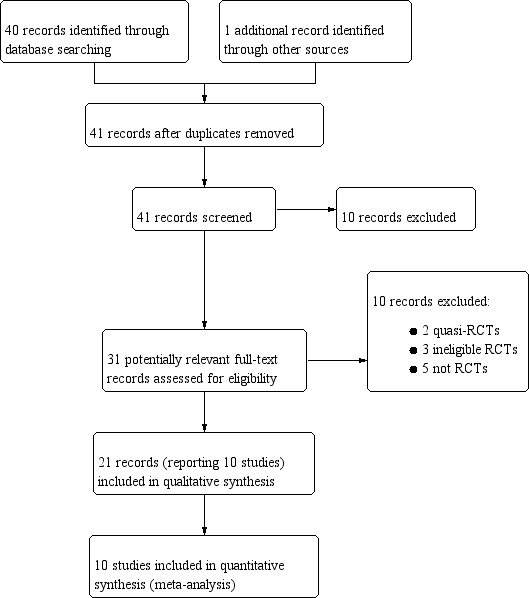
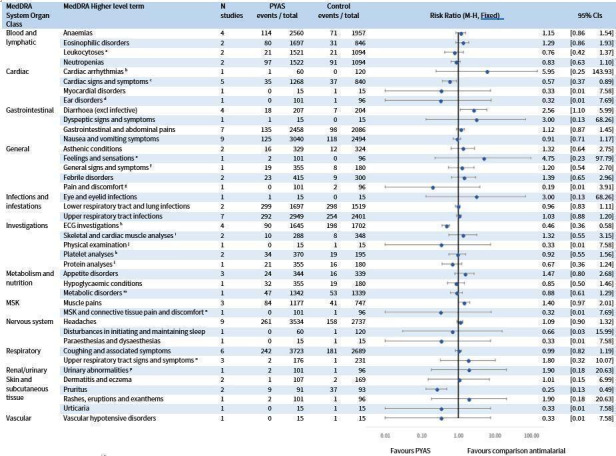
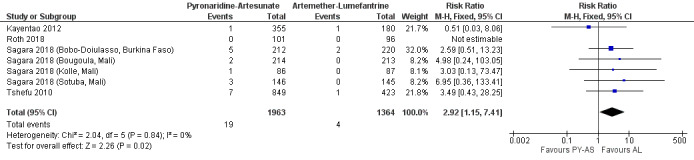
We included 10 relevant studies. Seven studies were co-funded by Shin Poong Pharmaceuticals which manufactures the drug. Three studies were funded by government agencies.For efficacy analysis we identified five RCTs with 5711 participants. This included 4465 participants from 13 sites in Africa, and 1246 participants from five sites in Asia. It included 541 children aged less than five years.For polymerase chain reaction (PCR)-adjusted failures at day 28, pyronaridine-artesunate may have fewer failures compared to artemether-lumefantrine (RR 0.59, 95% confidence interval (CI) 0.26 to 1.31; 4 RCTs, 3068 participants, low-certainty evidence), artesunate-amodiaquine (RR 0.55, 95% CI 0.11 to 2.77; 1 RCT, 1245 participants, low-certainty evidence), and mefloquine plus artesunate (RR 0.37, 95% CI 0.13 to 1.05; 1 RCT, 1117 participants, low-certainty evidence).For unadjusted failures at day 28, pyronaridine-artesunate may have fewer failures compared to artemether-lumefantrine (RR 0.27, 95% CI 0.13 to 0.58; 4 RCTs, 3149 participants, low-certainty evidence), and probably has fewer failures compared to artesunate-amodiaquine (RR 0.49, 95% CI 0.30 to 0.81; 1 RCT, 1257 participants, moderate-certainty evidence) and mefloquine plus artesunate (RR 0.36, 95% CI 0.17 to 0.78; 1 RCT, 1120 participants, moderate-certainty evidence).For PCR-adjusted failures at day 42, pyronaridine-artesunate may make little or no difference compared to artemether-lumefantrine (RR 0.86, 95% CI 0.49 to 1.51; 4 RCTs, 2575 participants, low-certainty evidence) and artesunate-amodiaquine (RR 0.98, 95% CI 0.20 to 4.83; 1 RCT, 1091 participants, low-certainty evidence), but may have higher failures than mefloquine plus artesunate (RR 1.80, 95% CI 0.90 to 3.57; 1 RCT, 1037 participants, low-certainty evidence). Overall, pyronaridine-artesunate had a PCR-adjusted treatment failure rate of less than 5%.For unadjusted failures at day 42, pyronaridine-artesunate may have fewer failures compared to artemether-lumefantrine (RR 0.61, 95% CI 0.46 to 0.82; 4 RCTs, 3080 participants, low-certainty evidence), may make little or no difference compared to mefloquine plus artesunate (RR 0.84, 95% CI 0.54 to 1.31; 1 RCT, 1059 participants, low-certainty evidence), and probably makes little or no difference compared to artesunate-amodiaquine (RR 0.98, 95% CI 0.78 to 1.23; 1 RCT, 1235 participants, moderate-certainty evidence).For the safety analysis of severe adverse events and liver function, we identified eight RCTs with 6614 participants comparing pyronaridine-artesunate to other antimalarials, four of which were not in the previous version of this review. A further two RCTs, comparing pyronaridine alone to other treatments, contributed to the synthesis of all adverse events.Raised alanine aminotransferase (ALT) greater than five times the upper limit of normal (> 5 x ULN) is more frequent with pyronaridine-artesunate compared to other antimalarials (RR 3.34, 95% CI 1.63 to 6.84; 8 RCTS, 6581 participants, high-certainty evidence). There is probably little or no difference for raised bilirubin > 2.5 x ULN between pyronaridine-artesunate and other antimalarials (RR 1.03, 95% CI 0.49 to 2.18; 7 RCTs, 6384 participants, moderate-certainty evidence). There was one reported case in which raised ALT occurred with raised bilirubin, meeting criteria for moderate drug-induced liver injury. No study reported severe drug-induced liver injury. Electrocardiograph (ECG) abnormalities were less common with pyronaridine-artesunate compared to other antimalarials. We identified no other safety concerns.
AUTHORS' CONCLUSIONS: Pyronaridine-artesunate was efficacious against uncomplicated P falciparum malaria, achieved a PCR-adjusted treatment failure rate of less than 5% at days 28 and 42, and may be at least as good as, or better than other marketed ACTs.Pyronaridine-artesunate increases the risk of episodes of raised ALT > 5 x ULN. This meets criteria for mild drug-induced liver injury. On one instance this was linked to raised bilirubin, indicating moderate drug-induced liver injury. No episodes of severe drug-induced liver injury were reported. The findings of this review cannot fully inform a risk-benefit assessment for an unselected population. Readers should remain aware of this uncertainty when considering use of pyronaridine-artesunate in patients with known or suspected pre-existing liver dysfunction, and when co-administering with other medications which may cause liver dysfunction.
世界卫生组织(WHO)推荐以青蒿素为基础的联合疗法(ACTs)治疗非复杂性恶性疟原虫疟疾。对青蒿素耐药性的担忧促使全球发起倡议,开发新的辅助药物以在ACT中保护青蒿素衍生物。双氢青蒿素哌喹是一种新型ACT。
评估双氢青蒿素哌喹与其他ACTs相比治疗非复杂性恶性疟原虫疟疾患者的疗效,以及评估双氢青蒿素哌喹和其他哌喹治疗与其他治疗相比的安全性。
我们检索了Cochrane传染病小组专业注册库;Cochrane图书馆中发表的Cochrane对照试验中心注册库(CENTRAL);MEDLINE;Embase;以及LILACS。我们还检索了ClinicalTrials.gov、WHO国际临床试验注册平台搜索门户以及国际标准随机对照试验编号(ISRCTN)注册库,以查找正在进行或最近完成的试验。最后一次检索日期为2018年5月8日。
疗效分析:双氢青蒿素哌喹治疗非复杂性恶性疟原虫疟疾的随机对照试验(RCTs)。安全性分析:双氢青蒿素哌喹或哌喹治疗恶性疟原虫或间日疟原虫疟疾的RCTs。
对于本次更新,两位综述作者独立重新提取所有数据并评估证据的确定性。我们对数据进行荟萃分析,以计算比较之间治疗失败的风险比(RRs),以及比较之间和跨比较的安全性结局的RRs。
我们纳入了10项相关研究。7项研究由生产该药物的信东制药共同资助。3项研究由政府机构资助。对于疗效分析,我们确定了5项RCTs,共5711名参与者。其中包括来自非洲13个地点的4465名参与者,以及来自亚洲5个地点的1246名参与者。包括541名5岁以下儿童。对于第28天经聚合酶链反应(PCR)调整的治疗失败,双氢青蒿素哌喹与蒿甲醚 - 本芴醇相比可能治疗失败更少(RR 0.59,95%置信区间(CI)0.26至1.31;4项RCTs,3068名参与者,低确定性证据),与青蒿琥酯 - 阿莫地喹相比(RR 0.55,95% CI 0.11至2.77;1项RCT,1245名参与者,低确定性证据),以及与甲氟喹加青蒿琥酯相比(RR 0.37,95% CI 0.13至1.05;1项RCT,1117名参与者低确定性证据)。对于第28天未经调整的治疗失败,双氢青蒿素哌喹与蒿甲醚 - 本芴醇相比可能治疗失败更少(RR 0.27,95% CI 0.13至0.58;4项RCTs,3 I49名参与者,低确定性证据),与青蒿琥酯 - 阿莫地喹相比可能治疗失败更少(RR 0.49,95% CI 0.30至0.81;1项RCT,1257名参与者,中度确定性证据),与甲氟喹加青蒿琥酯相比(RR 0.36,95% CI 0.17至0.78;1项RCT,1120名参与者,中度确定性证据)。对于第42天经PCR调整的治疗失败,双氢青蒿素哌喹与蒿甲醚 - 本芴醇相比可能差异不大或无差异(RR 0.86,95% CI 0.49至1.51;4项RCTs,2575名参与者,低确定性证据),与青蒿琥酯 - 阿莫地喹相比(RR 0.98,95% CI 0.20至4.83;1项RCT,1091名参与者,低确定性证据),但与甲氟喹加青蒿琥酯相比可能治疗失败更高(RR 1.80,95% CI 0.90至3.57;1项RCT,1037名参与者,低确定性证据)。总体而言,双氢青蒿素哌喹经PCR调整的治疗失败率低于5%。对于第42天未经调整的治疗失败,双氢青蒿素哌喹与蒿甲醚 - 本芴醇相比可能治疗失败更少(RR 0.61,95% CI 0.46至0.82;4项RCTs,3080名参与者,低确定性证据),与甲氟喹加青蒿琥酯相比可能差异不大或无差异(RR 0.84,95% CI 0.54至1.31;1项RCT,1059名参与者,低确定性证据),与青蒿琥酯 - 阿莫地喹相比可能差异不大或无差异(RR 0.98,95% CI 0.78至1.23;1项RCT,1235名参与者,中度确定性证据)。对于严重不良事件和肝功能的安全性分析,我们确定了8项RCTs,共6614名参与者,比较双氢青蒿素哌喹与其他抗疟药,其中4项不在本综述的上一版本中。另外2项RCTs,比较单独使用哌喹与其他治疗,有助于所有不良事件的综合分析。与其他抗疟药相比,双氢青蒿素哌喹导致丙氨酸氨基转移酶(ALT)升高超过正常上限5倍(>5×ULN)更为常见(RR 3.34,95% CI 1.63至6.84;8项RCTs,6581名参与者,高确定性证据)。双氢青蒿素哌喹与其他抗疟药相比,胆红素升高>2.5×ULN可能差异不大或无差异(RR 1.03,95% CI 0.49至2.18;7项RCTs,6384名参与者,中度确定性证据)。有1例报告病例,ALT升高同时伴有胆红素升高,符合中度药物性肝损伤标准。没有研究报告严重药物性肝损伤。与其他抗疟药相比,双氢青蒿素哌喹引起的心电图(ECG)异常较少见。我们未发现其他安全问题。
双氢青蒿素哌喹对非复杂性恶性疟原虫疟疾有效,在第28天和第42天经PCR调整的治疗失败率低于5%,可能至少与其他上市的ACTs一样好或更好。双氢青蒿素哌喹增加了ALT升高>5×ULN发作的风险。这符合轻度药物性肝损伤的标准。有1例这种情况与胆红素升高有关,表明为中度药物性肝损伤。未报告严重药物性肝损伤发作。本综述的结果不能完全为未选择人群的风险 - 效益评估提供信息。读者在考虑在已知或疑似存在肝功能障碍的患者中使用双氢青蒿素哌喹时,以及与其他可能导致肝功能障碍的药物合用时,应意识到这种不确定性。