Lee Yvonne C, Massarotti Elena, Edwards Robert R, Lu Bing, Liu ChihChin, Lo Yuanyu, Wohlfahrt Alyssa, Kim Nancy D, Clauw Daniel J, Solomon Daniel H
From the Division of Rheumatology, Immunology and Allergy, and Department of Anesthesiology, Brigham and Women's Hospital; Division of Rheumatology, Immunology and Allergy, Massachusetts General Hospital, Boston, Massachusetts; Department of Anesthesiology, University of Michigan Medical Center, Ann Arbor, Michigan, USA.Y.C. Lee, MD, MMSc, Division of Rheumatology, Department of Medicine, Brigham and Women's Hospital; E. Massarotti, MD, Division of Rheumatology, Brigham and Women's Hospital; R.R. Edwards, PhD, Pain Management Center, Brigham and Women's Hospital; B. Lu, MD, DrPH, Division of Rheumatology, Brigham and Women's Hospital; C. Liu, PhD, Division of Rheumatology, Brigham and Women's Hospital; Y. Lo, MPH, Division of Rheumatology, Brigham and Women's Hospital; A. Wohlfahrt, BA, Division of Rheumatology, Brigham and Women's Hospital; N.D. Kim, MD, Division of Rheumatology, Immunology and Allergy, Massachusetts General Hospital; D.J. Clauw, MD, University of Michigan; D.H. Solomon, MD, MPH, Division of Rheumatology, Brigham and Women's Hospital.
J Rheumatol. 2016 Jan;43(1):38-45. doi: 10.3899/jrheum.150550. Epub 2015 Dec 1.
Clinical trials have shown that serotonin norepinephrine reuptake inhibitors, such as milnacipran, decrease pain in noninflammatory pain conditions such as fibromyalgia and osteoarthritis. We examined the effect of milnacipran on self-reported pain intensity and experimental pain sensitivity among patients with rheumatoid arthritis (RA) with widespread pain and stable RA disease activity.
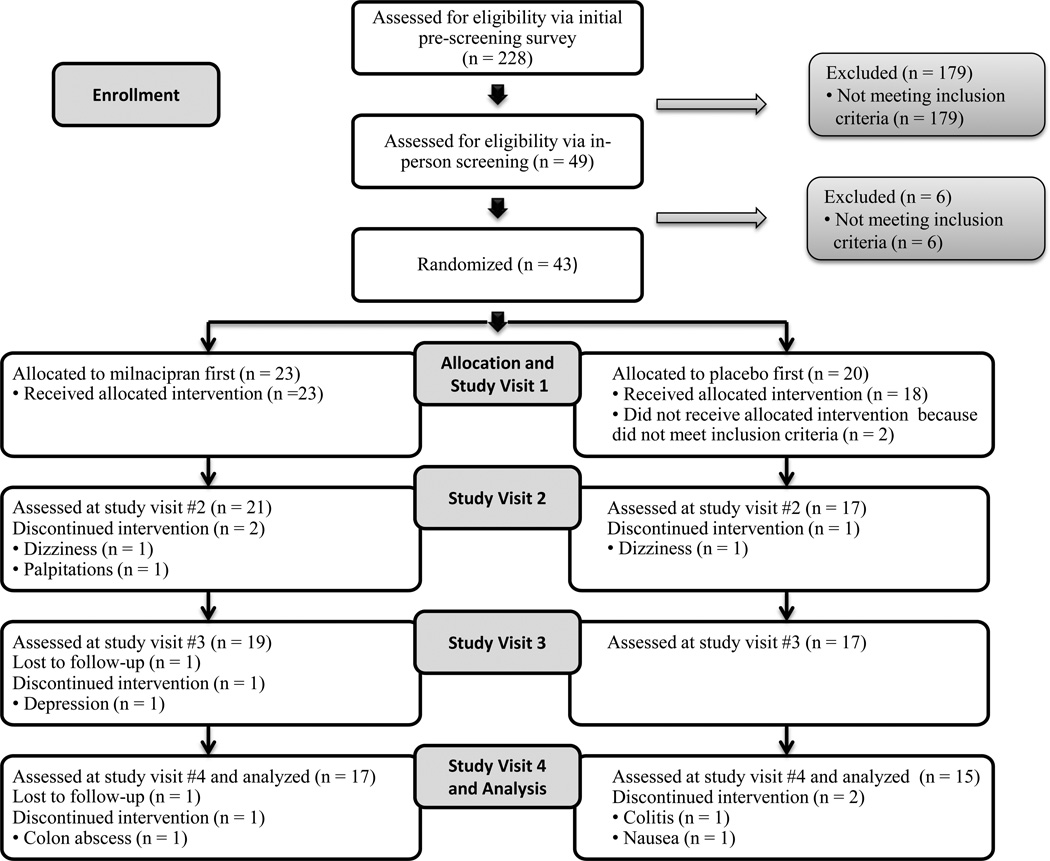
In this double-blind, crossover study, patients with RA with widespread pain, receiving a stable treatment regimen, were randomized (by a random number generator) to receive milnacipran 50 mg twice daily or placebo for 6 weeks, followed by a 3-week washout and crossed over to the other arm for the remaining 6 weeks. The primary outcome was change in average pain intensity, assessed by the Brief Pain Inventory short form. The sample size was calculated to detect a 30% improvement in pain with power = 0.80 and α = 0.05.
Of the 43 randomized subjects, 41 received the study drug, and 32 completed the 15-week study per protocol. On a 0-10 scale, average pain intensity decreased by 0.39 (95% CI -1.27 to 0.49, p = 0.37) more points during 6 weeks of milnacipran treatment compared with placebo. In the subgroup of subjects with swollen joint count ≤ 1, average pain intensity decreased by 1.14 more points during 6 weeks of milnacipran compared with placebo (95% CI -2.26 to -0.01, p = 0.04). Common adverse events included nausea (26.8%) and loss of appetite (9.7%).
Compared with placebo, milnacipran did not improve overall, self-reported pain intensity among subjects with widespread pain receiving stable RA medications.
ClinicalTrials.gov NCT01207453.
临床试验表明,血清素去甲肾上腺素再摄取抑制剂,如米那普明,可减轻纤维肌痛和骨关节炎等非炎性疼痛病症中的疼痛。我们研究了米那普明对患有广泛性疼痛且类风湿关节炎(RA)疾病活动稳定的患者自我报告的疼痛强度和实验性疼痛敏感性的影响。
在这项双盲、交叉研究中,患有广泛性疼痛且接受稳定治疗方案的RA患者被随机(通过随机数字生成器)分为两组,一组每天两次服用50毫克米那普明,另一组服用安慰剂,为期6周,随后有3周的洗脱期,然后交叉到另一组,再进行6周的治疗。主要结局是通过简明疼痛量表简表评估的平均疼痛强度变化。样本量的计算旨在检测疼痛改善30%,检验效能=0.80,α=0.05。
在43名随机分组的受试者中,41名接受了研究药物治疗,32名按照方案完成了15周的研究。在0至10分的量表上,与安慰剂相比,米那普明治疗6周期间平均疼痛强度降低了0.39分(95%置信区间为-1.27至0.49,p=0.37)。在关节肿胀计数≤1的受试者亚组中,与安慰剂相比,米那普明治疗6周期间平均疼痛强度降低了1.14分(95%置信区间为-2.26至-0.01,p=0.04)。常见的不良事件包括恶心(26.8%)和食欲不振(9.7%)。
与安慰剂相比,米那普明并未改善接受稳定RA药物治疗且患有广泛性疼痛的受试者总体的、自我报告的疼痛强度。
ClinicalTrials.gov NCT01207453。