Pasqua Franco, Nardi Ilaria, Provenzano Alessia, Mari Alessia
Pulmonary Medicine and Rehabilitation, Villa Delle Querce Hospital, Nemi, Rome Italy ; Pulmonary Rehabilitation, San Raffaele Hospital, Montecompatri, Rome Italy.
Pulmonary Medicine and Rehabilitation, Villa Delle Querce Hospital, Nemi, Rome Italy.
Multidiscip Respir Med. 2015 Nov 27;10:35. doi: 10.1186/s40248-015-0032-1. eCollection 2015.
Weaning from tracheostomy has implications in management, quality of life, and costs of ventilated patients. Furthermore, endotracheal cannula removing needs further studies. Aim of this study was the validation of a protocol for weaning from tracheostomy and evaluation of predictor factors of decannulation.
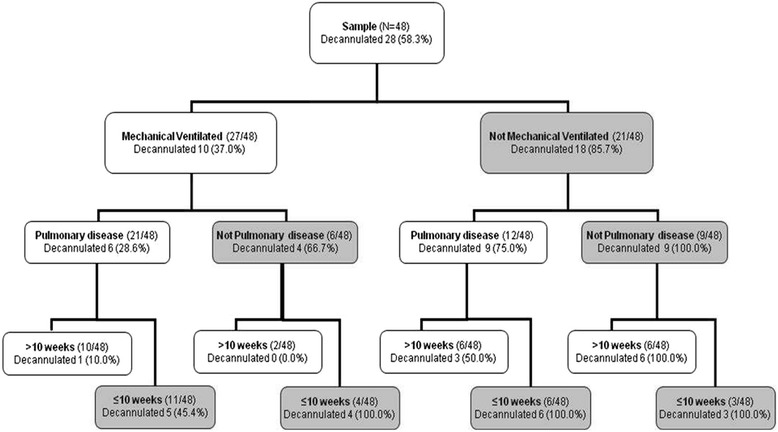
Medical records of 48 patients were retrospectively evaluated. Patients were decannulated in agreement with a decannulation protocol based on the evaluation of clinical stability, expiratory muscle strength, presence of tracheal stenosis/granulomas, deglutition function, partial pressure of CO2, and PaO2/FiO2 ratio. These variables, together with underlying disease, blood gas analysis parameters, time elapsed with cannula, comordibity, Barthel index, and the condition of ventilation, were evaluated in a logistic model as predictors of decannulation.
63 % of patients were successfully decannulated in agreement with our protocol and no one needed to be re-cannulated. Three variables were significantly associated with the decannulation: no pulmonary underlying diseases (OR = 7.12; 95 % CI 1.2-42.2), no mechanical ventilation (OR = 9.55; 95 % CI 2.1-44.2) and period of tracheostomy ≤10 weeks (OR = 6.5; 95 % CI 1.6-27.5).
The positive course of decannulated patients supports the suitability of the weaning protocol we propose here. The strong predictive role of three clinical variables gives premise for new studies testing simpler decannulation protocols.
气管造口术撤机对机械通气患者的管理、生活质量和成本均有影响。此外,气管插管拔除尚需进一步研究。本研究旨在验证气管造口术撤机方案并评估拔管的预测因素。
回顾性评估48例患者的病历。根据临床稳定性、呼气肌力量、气管狭窄/肉芽肿的存在、吞咽功能、二氧化碳分压和氧合指数(PaO2/FiO2)评估,按照撤管方案对患者进行拔管。在逻辑模型中评估这些变量以及基础疾病、血气分析参数、插管时间、合并症、巴氏指数和通气状况,作为拔管的预测因素。
63%的患者按照我们的方案成功拔管,且无人需要重新插管。三个变量与拔管显著相关:无肺部基础疾病(比值比[OR]=7.12;95%置信区间[CI]1.2 - 42.2)、无机械通气(OR = 9.55;95% CI 2.1 - 44.2)以及气管造口术时间≤10周(OR = 6.5;95% CI 1.6 - 27.5)。
拔管患者的良好过程支持了我们在此提出的撤机方案的适用性。三个临床变量的强大预测作用为测试更简单撤管方案的新研究提供了前提。