Ghiani Alessandro, Tsitouras Konstantinos, Paderewska Joanna, Milger Katrin, Walcher Swenja, Weiffenbach Mareike, Neurohr Claus, Kneidinger Nikolaus
Lung Center Stuttgart - Schillerhoehe Lung Clinic, Department of Pulmonology and Respiratory Medicine, Affiliated to the Robert-Bosch-Hospital GmbH, Auerbachstr. 110, 70376 Stuttgart, Germany.
Lung Center Stuttgart - Schillerhoehe Lung Clinic, Department of Pulmonology and Respiratory Medicine, Affiliated to the Robert-Bosch-Hospital GmbH, Stuttgart, Germany.
Ther Adv Chronic Dis. 2022 Aug 5;13:20406223221109655. doi: 10.1177/20406223221109655. eCollection 2022.
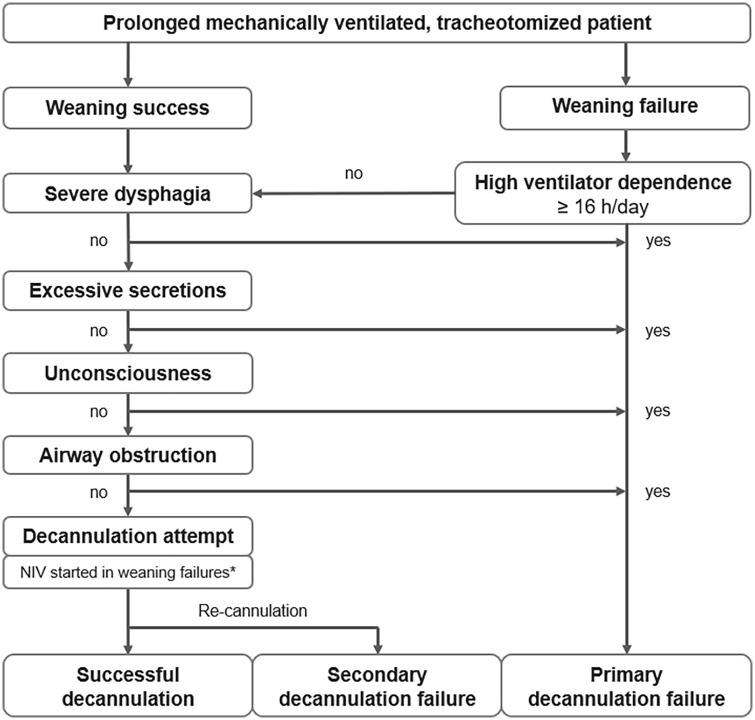
Liberation from prolonged tracheostomy ventilation involves ventilator weaning and removal of the tracheal cannula (referred to as decannulation). This study evaluated the incidence, causes, and predictors of unsuccessful decannulation following prolonged weaning.
Observational retrospective cohort study of 532 prolonged mechanically ventilated, tracheotomized patients treated at a specialized weaning center between June 2013 and January 2021. We summarized the causes for unsuccessful decannulations and used a binary logistic regression analysis to derive and validate associated predictors.
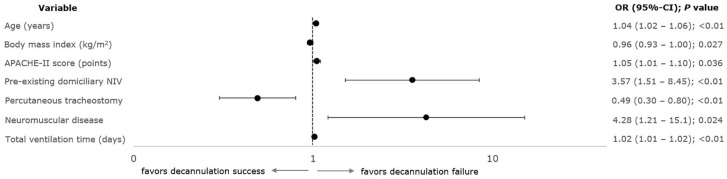
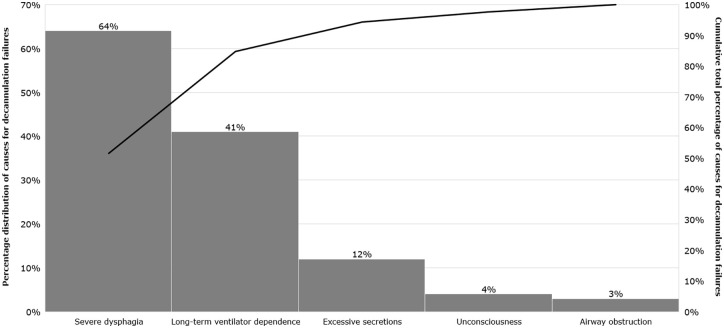
Failure to decannulate occurred in 216 patients (41%). The main causes were severe intensive care unit (ICU)-acquired dysphagia (64%), long-term ventilator dependence following weaning failure (41%), excessive respiratory secretions (12%), unconsciousness (4%), and airway obstruction (3%). Predictors of unsuccessful decannulation from any cause were age [odds ratio (OR) = 1.04 year; 95% confidence interval (CI), 1.02-1.06; < 0.01], body mass index [0.96 kg/m (0.93-1.00); = 0.027], Acute Physiology and Chronic Health Evaluation II (APACHE-II) score [1.05 (1.00-1.10); = 0.036], pre-existing non-invasive home ventilation [3.57 (1.51-8.45); < 0.01], percutaneous tracheostomies [0.49 (0.30-0.80); < 0.01], neuromuscular diseases [4.28 (1.21-15.1); = 0.024], and total mechanical ventilation duration [1.02 day (1.01-1.02); < 0.01]. Regression models examined in subsets of patients with severe dysphagia and long-term ventilator dependence as the main reason for failure revealed little overlapping among predictors, which even showed opposite effects on the outcome. The application of non-invasive ventilation as a weaning technique contributed to successful decannulation in 96 of 221 (43%) long-term ventilator-dependent patients following weaning failure.
Failure to decannulate after prolonged weaning occurred in 41%, mainly resulting from persistent ICU-acquired dysphagia and long-term ventilator dependence following weaning failure, each associated with its own set of predictors.
从长期气管切开通气中解放出来涉及呼吸机撤机和拔除气管套管(称为拔管)。本研究评估了长期撤机后拔管失败的发生率、原因及预测因素。
对2013年6月至2021年1月在一家专业撤机中心接受治疗的532例长期机械通气、气管切开患者进行观察性回顾性队列研究。我们总结了拔管失败的原因,并使用二元逻辑回归分析得出并验证相关预测因素。
216例患者(41%)拔管失败。主要原因是严重的重症监护病房(ICU)获得性吞咽困难(64%)、撤机失败后的长期呼吸机依赖(41%)、呼吸道分泌物过多(12%)、意识不清(4%)和气道阻塞(3%)。任何原因导致拔管失败的预测因素包括年龄[比值比(OR)=1.04岁;95%置信区间(CI),1.02 - 1.06;P<0.01]、体重指数[0.96kg/m²(0.93 - 1.00);P = 0.027]、急性生理与慢性健康状况评分II(APACHE-II)[1.05(1.00 - 1.10);P = 0.036]、既往无创家庭通气[3.57(1.51 - 8.45);P<0.01]、经皮气管切开术[0.49(0.30 - 0.80);P<0.01]、神经肌肉疾病[4.28(1.21 - 15.1);P = 0.024]以及机械通气总时长[1.02天(1.01 - 1.02);P<0.01]。在以严重吞咽困难和长期呼吸机依赖为主要失败原因的患者亚组中进行的回归模型分析显示,预测因素之间几乎没有重叠,甚至对结果显示出相反的影响。在221例撤机失败后长期依赖呼吸机的患者中,96例(43%)将无创通气作为撤机技术应用后成功拔管。
长期撤机后41%的患者拔管失败,主要原因是持续存在的ICU获得性吞咽困难和撤机失败后的长期呼吸机依赖,且每种情况都有其各自的一组预测因素。