Sharma Monisha, Ying Roger, Tarr Gillian, Barnabas Ruanne
Department of Epidemiology, University of Washington, 1959 NE Pacific Street, Seattle, Washington 98195, USA.
Department of Global Health, University of Washington, 1510 San Juan Road 310e, Seattle, Washington 98195, USA.
Nature. 2015 Dec 3;528(7580):S77-85. doi: 10.1038/nature16044.
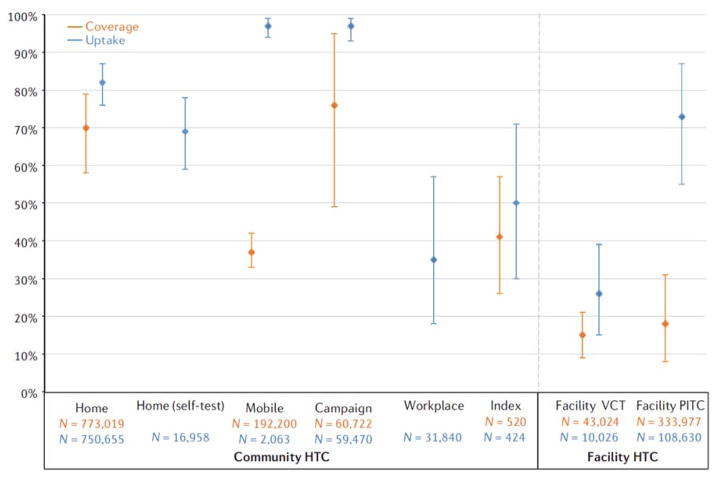
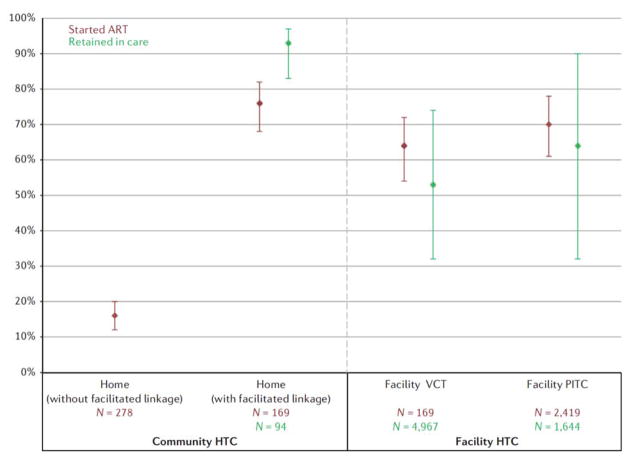
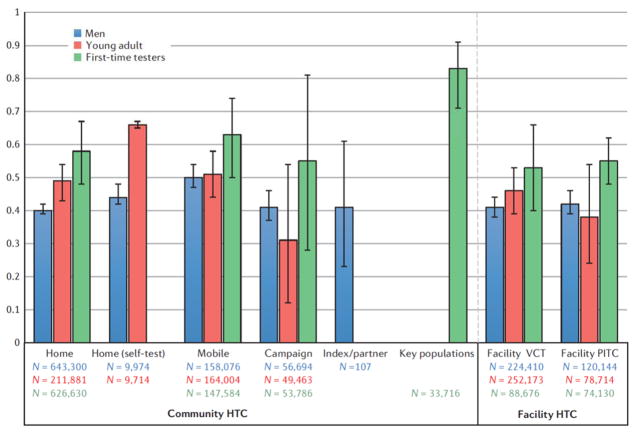
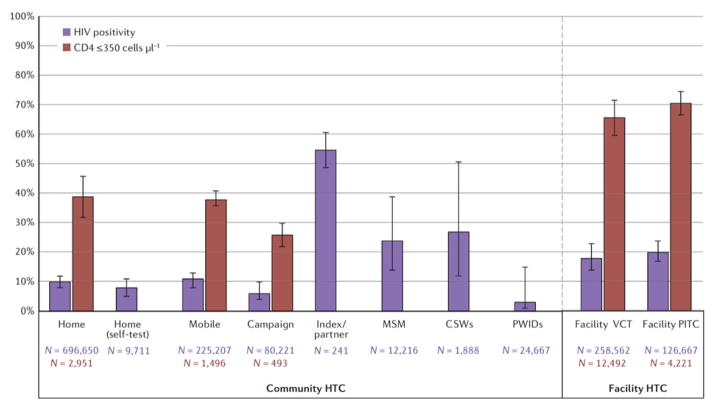
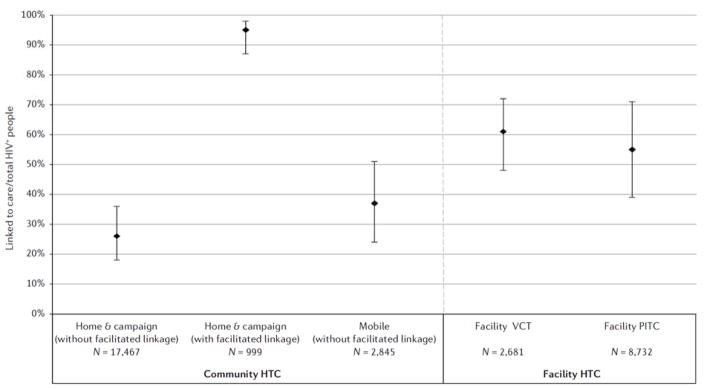
HIV testing and counselling is the first crucial step for linkage to HIV treatment and prevention. However, despite high HIV burden in sub-Saharan Africa, testing coverage is low, particularly among young adults and men. Community-based HIV testing and counselling (testing outside of health facilities) has the potential to reduce coverage gaps, but the relative impact of different modalities is not well assessed. We conducted a systematic review of HIV testing modalities, characterizing community (home, mobile, index, key populations, campaign, workplace and self-testing) and facility approaches by population reached, HIV positivity, CD4 count at diagnosis and linkage. Of 2,520 abstracts screened, 126 met eligibility criteria. Community HIV testing and counselling had high coverage and uptake and identified HIV-positive people at higher CD4 counts than facility testing. Mobile HIV testing reached the highest proportion of men of all modalities examined (50%, 95% confidence interval (CI) = 47-54%) and home with self-testing reached the highest proportion of young adults (66%, 95% CI = 65-67%). Few studies evaluated HIV testing for key populations (commercial sex workers and men who have sex with men), but these interventions yielded high HIV positivity (38%, 95% CI = 19-62%) combined with the highest proportion of first-time testers (78%, 95% CI = 63-88%), indicating service gaps. Community testing with facilitated linkage (for example, counsellor follow-up to support linkage) achieved high linkage to care (95%, 95% CI = 87-98%) and antiretroviral initiation (75%, 95% CI = 68-82%). Expanding home and mobile testing, self-testing and outreach to key populations with facilitated linkage can increase the proportion of men, young adults and high-risk individuals linked to HIV treatment and prevention, and decrease HIV burden.
艾滋病毒检测与咨询是与艾滋病毒治疗和预防建立联系的关键第一步。然而,尽管撒哈拉以南非洲地区艾滋病毒负担沉重,但检测覆盖率较低,尤其是在年轻人和男性中。基于社区的艾滋病毒检测与咨询(在医疗机构之外进行检测)有可能缩小覆盖率差距,但不同方式的相对影响尚未得到充分评估。我们对艾滋病毒检测方式进行了系统评价,按覆盖人群、艾滋病毒阳性率、诊断时的CD4细胞计数和转介情况对社区(家庭、流动、索引、重点人群、宣传活动、工作场所和自我检测)和医疗机构检测方式进行了描述。在筛选的2520篇摘要中,126篇符合纳入标准。社区艾滋病毒检测与咨询覆盖率和接受率较高,确诊时艾滋病毒阳性者的CD4细胞计数高于医疗机构检测。在所有检测方式中,流动艾滋病毒检测覆盖的男性比例最高(50%,95%置信区间(CI)=47-54%);家庭自我检测覆盖的年轻人比例最高(66%,95%CI=65-67%)。很少有研究评估针对重点人群(商业性工作者和男男性行为者)的艾滋病毒检测,但这些干预措施的艾滋病毒阳性率较高(38%,95%CI=19-62%),首次检测者的比例也最高(78%,95%CI=63-88%),表明存在服务差距。通过便利转介进行社区检测(例如,咨询师跟进以支持转介)实现了较高的治疗衔接率(95%,95%CI=87-98%)和抗逆转录病毒治疗启动率(75%,95%CI=68-82%)。扩大家庭和流动检测、自我检测,并通过便利转介向重点人群提供外展服务,可以增加与艾滋病毒治疗和预防建立联系的男性、年轻人和高危个体的比例,并减轻艾滋病毒负担。