Fragulidis Georgios Panagiotis, Vezakis Antonios I, Kontis Elissaios A, Pantiora Eirini V, Stefanidis Gerasimos G, Politi Aikaterini N, Koutoulidis Vasilios K, Mela Maria K, Polydorou Andreas A
From the 2nd Department of Surgery, Aretaieio Hospital, University of Athens, Medical School (GPF, AIV, EAK, EVP, AAP); Department of Gastroenterology, Division of Endoscopy, Athens Naval Hospital (GGS); Department of Pathology, Aretaieio Hospital, University of Athens, Medical School (ANP); 1st Department of Radiology, Aretaieio Hospital, University of Athens, Medical School (VKK); and Department of Hepatology, Evangelismos General Hospital, Athens, Greece (MKM).
Medicine (Baltimore). 2016 Jan;95(1):e2394. doi: 10.1097/MD.0000000000002394.
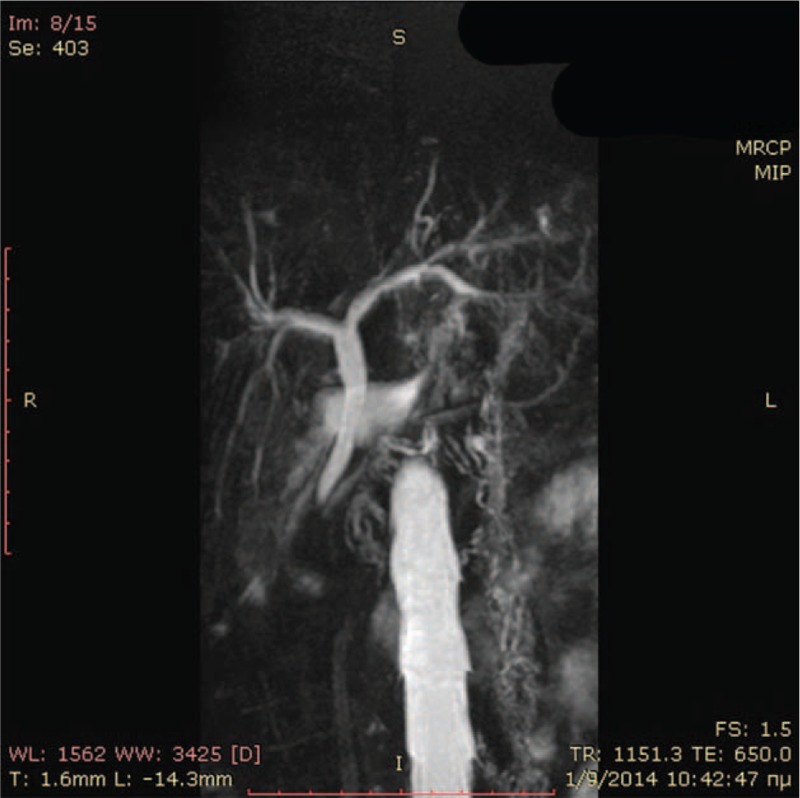
When confronting a biliary stricture, both benign and malignant etiologies must be carefully considered as a variety of benign biliary strictures can masquerade as hilar cholangiocarcinoma (CCA). Therefore, patients could undergo a major surgery despite the possibility of a benign biliary disease. Approximately 15% to 24% of patients undergoing surgical resection for suspected biliary malignancy will have benign pathology. Eosinophilic cholangitis (EC) is a rare benign disorder of the biliary tract, which can cause obstructive jaundice and can pose a difficult diagnostic task. We present a rare case of a young woman who was referred to our hospital with obstructive painless jaundice due to a biliary stricture at the confluence of the hepatic bile ducts, with a provisional diagnosis of cholangiocarcinoma. Though, during her work up she was found to have EC, an extremely rare benign cause of biliary stricture, which is characterized by a dense eosinophilic infiltration of the biliary tree causing stricturing, fibrosis, and obstruction and which is reversible with short-term high-dose steroids. Despite its rarity, EC should be taken into consideration when imaging modalities demonstrate a biliary stricture, especially if preoperative diagnosis of malignancy cannot be made, in the setting of peripheral eosinophilia and the absence of cardinal symptoms of malignancy.
面对胆管狭窄时,必须仔细考虑良性和恶性病因,因为多种良性胆管狭窄可能会伪装成肝门部胆管癌(CCA)。因此,尽管可能是良性胆道疾病,患者仍可能接受大手术。在因疑似胆道恶性肿瘤而接受手术切除的患者中,约15%至24%会有良性病理结果。嗜酸性胆管炎(EC)是一种罕见的胆道良性疾病,可导致梗阻性黄疸,并且可能带来诊断难题。我们报告一例罕见病例,一名年轻女性因肝内胆管汇合处胆管狭窄导致梗阻性无痛性黄疸被转诊至我院,初步诊断为胆管癌。然而,在检查过程中发现她患有EC,这是一种极其罕见的胆管狭窄良性病因,其特征是胆管树有密集的嗜酸性粒细胞浸润,导致狭窄、纤维化和梗阻,并且短期高剂量使用类固醇激素可使其逆转。尽管EC罕见,但当影像学检查显示胆管狭窄时,尤其是在无法做出术前恶性肿瘤诊断、存在外周嗜酸性粒细胞增多且无恶性肿瘤主要症状的情况下,应考虑到EC。