Montgomery Agneta, Kallinowski Friedrich, Köckerling Ferdinand
Department of Surgery, Skane University Hospital , Malmö , Sweden.
Department of Surgery, Asklepios Hospital Harburg , Hamburg , Germany.
Front Surg. 2016 Jan 8;2:67. doi: 10.3389/fsurg.2015.00067. eCollection 2015.
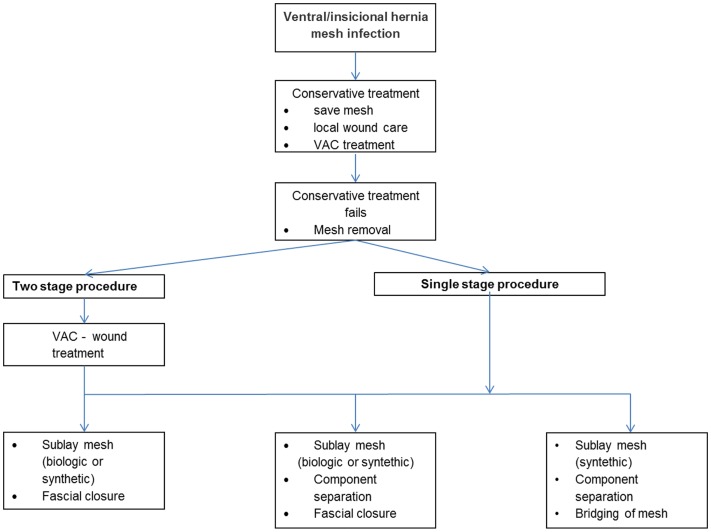
The incidence of deep infection using a synthetic mesh in inguinal hernia repair is low and reported to be well below 1%. This is in contrast to incisional hernia surgery where the reported incidence is 3% respective 13% comparing laparoscopic to open mesh repair reported in a Cochrane review. Main risk factors were long operation time, surgical site contamination, and early wound complications. An infected mesh can be preserved using conservative treatment were negative pressure wound therapy (VAC(®)) could play an important role. If strategy fails, the mesh needs to be removed. This review aims to look at evidence for situations were a biological mesh would work as a replacement of a removed infected synthetic mesh.
A literature search of the Medline database was performed using the PubMed search engine. Twenty publications were found relevant for this review.
For studies reviewed three options are presented: removal of the infected synthetic mesh alone, replacement with either a new synthetic or a new biological mesh. Operations were all performed at specialist centers. Removal of the mesh alone was an option limited to inguinal hernias. In ventral/incisional hernias, the use of a biological mesh for replacement resulted in a very high recurrence rate, if bridging was required. Either a synthetic or a biological mesh seems to work as a replacement when fascial closure can be achieved. Evidence is though very low.
When required, either a synthetic or a biological mesh seems to work as a replacement for an infected synthetic mesh if the defect can be closed. It is, however, not recommended to use a biological mesh for bridging. Mesh replacement surgery is demanding and is recommended to be performed in a specialist center.
在腹股沟疝修补术中使用合成补片发生深部感染的发生率较低,据报道远低于1%。这与切口疝手术形成对比,在一项Cochrane综述中,腹腔镜与开放补片修补术相比,切口疝手术报道的发生率分别为3%和13%。主要危险因素包括手术时间长、手术部位污染和早期伤口并发症。对于感染的补片,采用保守治疗(负压伤口治疗(VAC(®))可能发挥重要作用)可保留补片。如果该策略失败,则需要取出补片。本综述旨在探讨生物补片可替代取出的感染合成补片的证据。
使用PubMed搜索引擎对Medline数据库进行文献检索。共找到20篇与本综述相关的出版物。
对于所综述的研究,提出了三种选择:仅取出感染的合成补片、用新的合成补片或新的生物补片进行替换。所有手术均在专科中心进行。仅取出补片这一选择仅限于腹股沟疝。在腹侧/切口疝中,如果需要桥接,使用生物补片进行替换会导致非常高的复发率。当能够实现筋膜闭合时,合成补片或生物补片似乎都可作为替代品。不过证据非常有限。
如果缺损能够闭合,在需要时,合成补片或生物补片似乎都可替代感染的合成补片。然而,不建议使用生物补片进行桥接。补片置换手术要求较高,建议在专科中心进行。