Milan Manani Sabrina, Virzì Grazia Maria, Clementi Anna, Brocca Alessandra, de Cal Massimo, Tantillo Ilaria, Ferrando Lorena, Crepaldi Carlo, Ronco Claudio
Department of Nephrology, Dialysis and Transplant, San Bortolo Hospital, Vicenza, Italy; IRRIV-International Renal Research Institute, Vicenza, Italy.
IRRIV-International Renal Research Institute, Vicenza, Italy; Department of Nephrology and Dialysis, San Giovanni Di Dio Hospital, Cagliari, Italy.
Clin Kidney J. 2016 Feb;9(1):153-7. doi: 10.1093/ckj/sfv137. Epub 2015 Dec 13.
Inflammation and serum albumin concentration are both important predictors of survival in patients treated with peritoneal dialysis (PD). Furthermore, systemic and local inflammatory mediators may induce structural and functional alterations in the peritoneal membrane, thus interfering with dialysis adequacy. PD adequacy is monitored primarily by indices of small solute clearance, such as Kt/V urea and weekly creatinine clearance (wCc). The aim of this study was to investigate the possible relationship between pro-inflammatory cytokines, such as interleukin-6 (IL-6) and interleukin-1β (IL-1β), and serum albumin and C-reactive protein (CRP). Moreover, the relationship between IL-6 and IL-1β and PD adequacy has been analysed.
We enrolled 46 stable PD patients undergoing maintenance PD for a minimum of 3 months. Plasma levels of serum albumin, high-sensitivity (hs)-CRP, IL-6 and IL-1β were measured in all patients. We used weekly Kt/V urea and wCc to monitor PD adequacy. Daily urine volume was measured in all patients.
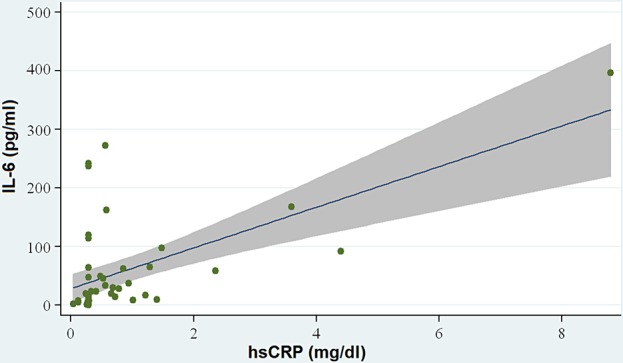
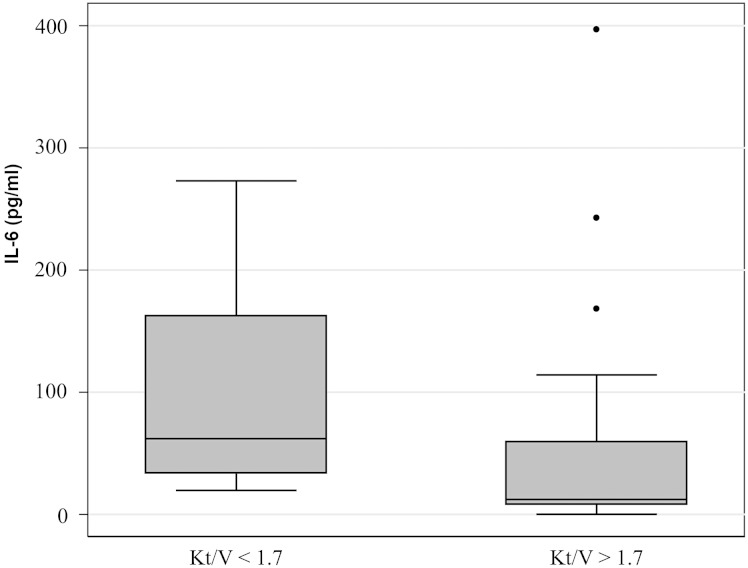
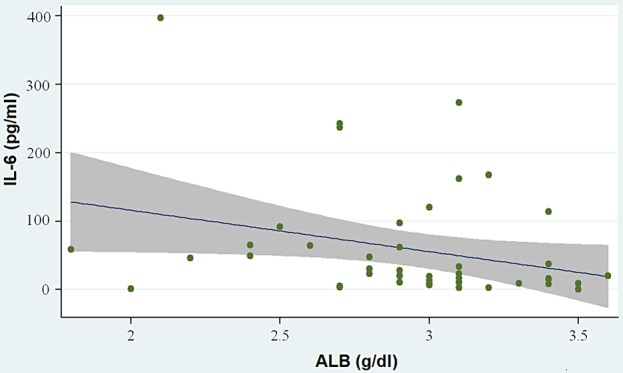
The median values of serum albumin, hs-CRP, IL-6 and IL-1β showed no significant differences between continuous ambulatory PD and automated PD patients. IL-6 levels showed a positive correlation with hs-CRP levels (P < 0.001) and a negative correlation with serum albumin concentration (P = 0.01). There was no statistically significant relationship between IL-1β and hs-CRP or serum albumin concentrations. Subsequently, PD patients were divided into two groups based on Kt/V urea value. PD patients with Kt/V ≤1.7 had significantly higher IL-6 levels compared with PD patients with Kt/V >1.7 (P = 0.015). No statistically significant relationship between IL-6 and wCc was observed. There was no significant difference in IL-1β levels between PD patients with Kt/V ≤1.7 and with Kt/V >1.7 [median (interquartile range) 0.82 (0.88-5.2) versus 1.82 (0.95-2.7)]. There was no significant difference in IL-6 and IL-1β levels in PD patients with and without residual diuresis (P = 0.32 and P = 0.77, respectively).
Our data suggest a possible relationship between serum IL-6 levels and serum albumin and hs-CRP in PD patients. Furthermore, IL-6 seems to be higher in patients with lower Kt/V, thus suggesting a possible use of this inflammatory biomarker in PD adequacy monitoring.
炎症反应和血清白蛋白浓度都是接受腹膜透析(PD)治疗患者生存的重要预测指标。此外,全身和局部炎症介质可能会引起腹膜结构和功能改变,进而影响透析充分性。PD充分性主要通过小分子溶质清除指标进行监测,如尿素Kt/V和每周肌酐清除率(wCc)。本研究旨在探讨促炎细胞因子,如白细胞介素-6(IL-6)和白细胞介素-1β(IL-1β),与血清白蛋白和C反应蛋白(CRP)之间可能存在的关系。此外,还分析了IL-6和IL-1β与PD充分性之间的关系。
我们纳入了46例接受维持性PD至少3个月的稳定PD患者。测定了所有患者血浆中的血清白蛋白、高敏(hs)-CRP、IL-6和IL-1β水平。我们使用每周尿素Kt/V和wCc来监测PD充分性。测定了所有患者的每日尿量。
连续非卧床PD患者和自动化PD患者之间,血清白蛋白、hs-CRP、IL-6和IL-1β的中位数无显著差异。IL-6水平与hs-CRP水平呈正相关(P < 0.001),与血清白蛋白浓度呈负相关(P = 0.01)。IL-1β与hs-CRP或血清白蛋白浓度之间无统计学显著关系。随后,根据尿素Kt/V值将PD患者分为两组。Kt/V≤1.7的PD患者IL-6水平显著高于Kt/V>1.7的PD患者(P = 0.015)。未观察到IL-6与wCc之间有统计学显著关系。Kt/V≤1.7和Kt/V>1.7的PD患者IL-1β水平无显著差异[中位数(四分位间距)0.82(0.88 - 5.2)对1.82(0.95 - 2.7)]。有残余尿量和无残余尿量的PD患者IL-6和IL-水平无显著差异(分别为P = 0.32和P = 0.77)。
我们的数据表明PD患者血清IL-6水平与血清白蛋白和hs-CRP之间可能存在关系。此外,Kt/V较低患者的IL-6似乎更高,因此提示该炎症生物标志物可能用于监测PD充分性。