Grimshaw Kate E C, Bryant Trevor, Oliver Erin M, Martin Jane, Maskell Joe, Kemp Terri, Clare Mills E N, Foote Keith D, Margetts Barrie M, Beyer Kirsten, Roberts Graham
Clinical and Experimental Sciences and Human Development in Health Academic Unit, Faculty of Medicine, University of Southampton, Mailpoint 803, Level F, South Academic Block, Southampton, SO16 6YD UK ; Department of Nutrition and Dietetics, Southampton Children's Hospital, Southampton, SO16 6YD UK.
Primary Care and Population Sciences Academic Unit, Faculty of Medicine, University of Southampton, Southampton, SO16 6YD UK.
Clin Transl Allergy. 2016 Jan 26;6:1. doi: 10.1186/s13601-016-0089-8. eCollection 2015.
The prevalence of food hypersensitivity in the UK is still largely open to debate. Additionally its pathogenesis is also unclear although it is known that there are differing phenotypes. Determining its prevalence, along with identifying those factors associated with its development will help to assess its clinical importance within the national setting and also add to the debate on appropriate prevention strategies.
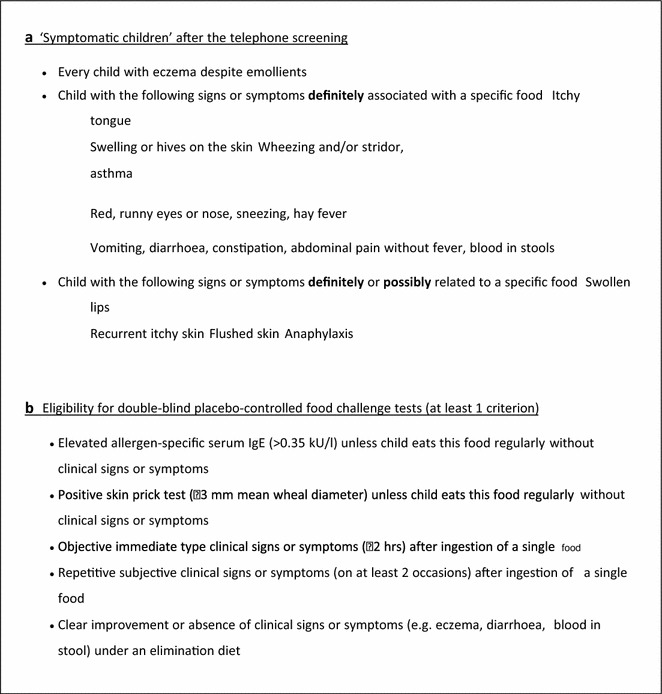
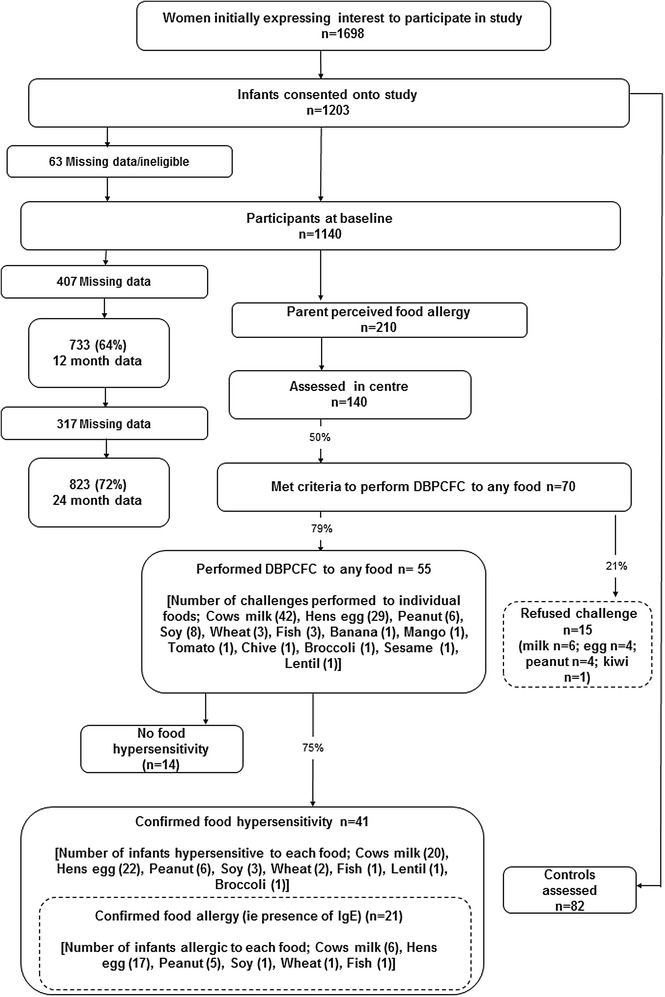
A population based birth cohort study conducted in Hampshire, UK as part of the EuroPrevall birth cohort study. 1140 infants were recruited with 823 being followed up until 2 years of age. Infants with suspected food reactions were assessed including specific IgE measurement and skin prick testing. Diagnosis of food hypersensitivity was by positive double-blind, placebo-controlled food challenge (DBPCFC) where symptoms up to 48 h after the end of the food challenge were considered indicative of a food hypersensitivity. Factors associated with food hypersensitivity and its two phenotypes of IgE-mediated and non-IgE-mediated disease were modelled in a multivariable logistic regression analysis.
Cumulative incidence of food hypersensitivity by 2 years of age was 5.0 %. The cumulative incidence for individual food allergens were hens' egg 2.7 % (1.6-3.8); cows' milk 2.4 % (1.4-3.5); peanut 0.7 % (0.1-1.3); soy 0.4 % (0.0-0.8); wheat 0.2 % (0.0-0.5) and 0.1 % (0.0-0.32) for fish. The cumulative incidence of IgE-mediated food allergy was 2.6 % with 2.1 % reacting to hens' egg. For non-IgE-mediated food allergy the cumulative incidence was 2.4 % (cows' milk 1.7 %). Predictors for any food hypersensitivity were wheeze, maternal atopy, increasing gestational age, age at first solid food introduction and mean healthy dietary pattern score. Predictors for IgE mediated allergy were eczema, rhinitis and healthy dietary pattern score whereas for non-IgE-mediated food allergy the predictors were dog in the home, healthy dietary pattern score, maternal consumption of probiotics during breastfeeding and age at first solid food introduction.
Just under half the infants with confirmed food hypersensitivity had no demonstrable IgE. In an exploratory analysis, risk factors for this phenotype of food hypersensitivity differed from those for IgE-mediated food allergy except for a healthy infant diet which was associated with less risk for both phenotypes.
英国食物过敏的患病率仍存在很大争议。此外,尽管已知存在不同的表型,但其发病机制也尚不清楚。确定其患病率以及识别与疾病发展相关的因素,将有助于评估其在全国范围内的临床重要性,并为有关适当预防策略的辩论提供补充。
作为欧洲PrevALL出生队列研究的一部分,在英国汉普郡进行了一项基于人群的出生队列研究。招募了1140名婴儿,其中823名随访至2岁。对疑似食物反应的婴儿进行了评估,包括特异性IgE测量和皮肤点刺试验。食物过敏的诊断采用阳性双盲、安慰剂对照食物激发试验(DBPCFC),食物激发试验结束后48小时内出现的症状被视为食物过敏的指征。在多变量逻辑回归分析中,对与食物过敏及其IgE介导和非IgE介导疾病的两种表型相关的因素进行建模。
2岁时食物过敏的累积发病率为5.0%。个别食物过敏原的累积发病率分别为:鸡蛋2.7%(1.6 - 3.8);牛奶2.4%(1.4 - 3.5);花生0.7%(0.1 - 1.3);大豆0.4%(0.0 - 0.8);小麦0.2%(0.0 - 0.5);鱼类0.1%(0.0 - 0.32)。IgE介导的食物过敏累积发病率为2.6%,其中2.1%对鸡蛋有反应。非IgE介导的食物过敏累积发病率为2.4%(牛奶为1.7%)。任何食物过敏的预测因素为喘息、母亲过敏体质、孕周增加、首次引入固体食物的年龄和平均健康饮食模式评分。IgE介导过敏的预测因素为湿疹、鼻炎和健康饮食模式评分,而非IgE介导食物过敏的预测因素为家中养狗、健康饮食模式评分、母亲在母乳喂养期间食用益生菌以及首次引入固体食物的年龄。
确诊食物过敏的婴儿中,近一半没有可证实的IgE。在一项探索性分析中除了健康的婴儿饮食与两种表型的风险降低相关外,这种食物过敏表型的危险因素与IgE介导的食物过敏不同。