Macaulay Valentine M, Middleton Mark R, Eckhardt S Gail, Rudin Charles M, Juergens Rosalyn A, Gedrich Richard, Gogov Sven, McCarthy Sean, Poondru Srinivasu, Stephens Andrew W, Gadgeel Shirish M
University Department of Oncology, Oxford Cancer and Haematology Centre, Headington, Oxford, United Kingdom.
University of Colorado Cancer Center, Aurora, Colorado.
Clin Cancer Res. 2016 Jun 15;22(12):2897-907. doi: 10.1158/1078-0432.CCR-15-2218. Epub 2016 Feb 1.
Cross-talk between type I IGF receptor (IGF1R), insulin receptor (INSR), and epidermal growth factor receptor (EGFR) mediates resistance to individual receptor blockade. This study aimed to determine the MTD, safety, pharmacokinetics, pharmacodynamics, and preliminary antitumor activity of linsitinib, a potent oral IGF1R/INSR inhibitor, with EGFR inhibitor erlotinib.
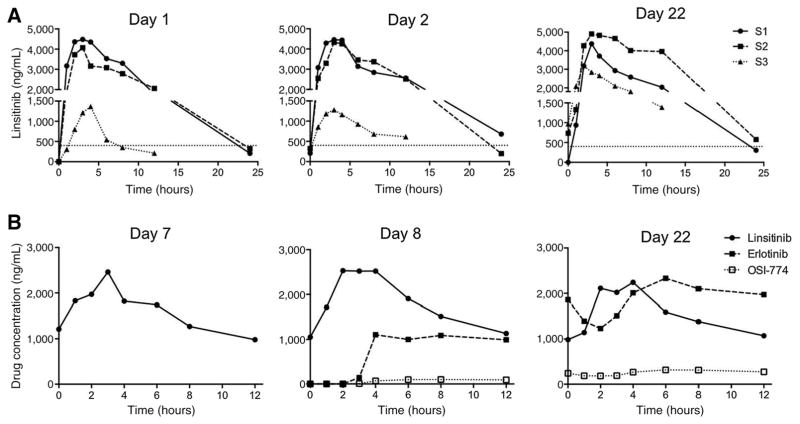
This open-label, dose-escalation study investigated linsitinib schedules S1: once daily intermittent (days 1-3 weekly); S2, once daily continuous; S3, twice-daily continuous; each with erlotinib 100-150 mg once daily; and a non-small cell lung cancer (NSCLC) expansion cohort.
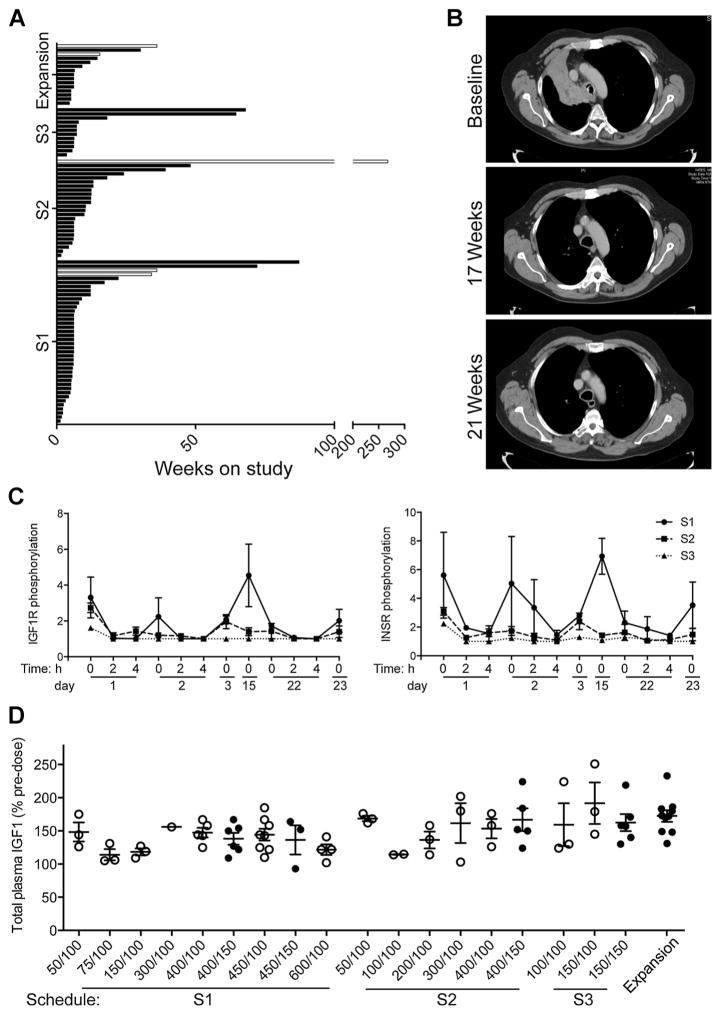
Ninety-five patients were enrolled (S1, 44; S2, 24; S3, 12; expansion cohort, 15) and 91 treated. Seven experienced dose-limiting toxicities: QTc prolongation (3), abnormal liver function (2), hyperglycemia (1), and anorexia (1). Common adverse events included drug eruption (84%), diarrhea (73%), fatigue (68%), nausea (58%), vomiting (40%). MTDs for linsitinib/erlotinib were 450/150 mg (S1), 400/100 mg (S2). On the basis of prior monotherapy data, S3 dosing at 150 mg twice daily/150 mg once daily was the recommended phase II dose for the expansion cohort. There was no evidence of drug-drug interaction. Pharmacodynamic data showed IGF-1 elevation and reduced IGF1R/INSR phosphorylation, suggesting pathway inhibition. Across schedules, 5/75 (7%) evaluable patients experienced partial responses: spinal chordoma (268+ weeks), rectal cancer (36 weeks), three NSCLCs including 2 adenocarcinomas (16, 72 weeks), 1 squamous wild-type EGFR NSCLC (36 weeks). Disease control (CR+PR+SD) occurred in 38 of 75 (51%), and 28 of 91 (31%) patients were on study >12 weeks.
The linsitinib/erlotinib combination was tolerable with preliminary evidence of activity, including durable responses in cases unlikely to respond to erlotinib monotherapy. Clin Cancer Res; 22(12); 2897-907. ©2016 AACR.
I型胰岛素样生长因子受体(IGF1R)、胰岛素受体(INSR)和表皮生长因子受体(EGFR)之间的相互作用介导了对单个受体阻断的耐药性。本研究旨在确定强效口服IGF1R/INSR抑制剂林西替尼与EGFR抑制剂厄洛替尼联合使用时的最大耐受剂量(MTD)、安全性、药代动力学、药效学及初步抗肿瘤活性。
本开放标签、剂量递增研究考察了林西替尼的给药方案:方案S1:每日一次间歇给药(每周第1 - 3天);方案S2,每日一次连续给药;方案S3,每日两次连续给药;每种方案均联合每日一次100 - 150 mg厄洛替尼;并设立了非小细胞肺癌(NSCLC)扩展队列。
共入组95例患者(方案S1,44例;方案S2,24例;方案S3,12例;扩展队列,15例),91例接受治疗。7例出现剂量限制性毒性:QTc延长(3例)、肝功能异常(2例)、高血糖(1例)和厌食(1例)。常见不良事件包括药疹(84%)、腹泻(73%)、疲劳(68%)、恶心(58%)、呕吐(40%)。林西替尼/厄洛替尼的MTD分别为方案S1:450/150 mg,方案S2:400/100 mg。根据既往单药治疗数据,扩展队列的推荐II期剂量为方案S3:每日两次150 mg/每日一次150 mg。未发现药物相互作用的证据。药效学数据显示IGF - 1升高,IGF1R/INSR磷酸化降低,提示通路受到抑制。在所有给药方案中,75例可评估患者中有5例(7%)出现部分缓解:脊索瘤(268 +周)、直肠癌(36周)、3例NSCLC,包括2例腺癌(16、72周)、1例鳞状野生型EGFR NSCLC(36周)。75例患者中有38例(51%)疾病得到控制(完全缓解+部分缓解+疾病稳定),91例患者中有28例(31%)研究时间>12周。
林西替尼/厄洛替尼联合用药耐受性良好,有初步的活性证据,包括在不太可能对厄洛替尼单药治疗产生反应的病例中出现持久缓解。《临床癌症研究》;22(12);2897 - 907。©2016美国癌症研究协会。