Department of Medicine , Khon Kaen University , Khon Kaen , Thailand.
Department of Medicine , Khon Kaen Regional Hospital , Khon Kaen , Thailand.
Lupus Sci Med. 2016 Jan 14;3(1):e000120. doi: 10.1136/lupus-2015-000120. eCollection 2016.
The optimal treatment of relapse or resistant lupus nephritis (LN) is still unclear. Mycophenolate might be an alternative therapy to avoid toxicities of cyclophosphamide (CYC). This study was aimed to compare enteric-coated mycophenolate sodium (EC-MPS) versus intravenous CYC as an induction therapy.
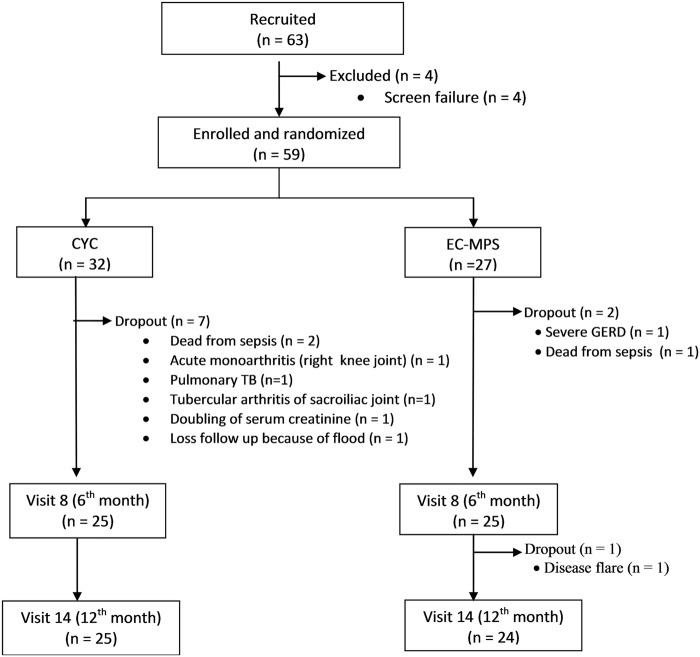
The study was a 12-month period of multicentre, open-labelled randomised controlled trial. Fifty-nine patients who had relapsed (36%) or who were resistant to previous CYC treatment (64%) and all who were biopsy-proven class III/IV, were randomised into CYC (n=32) and EC-MPS groups (n=27). The CYC group received intravenous CYC 0.5-1 g/m(2) monthly and the EC-MPS group was treated with EC-MPS 1440 mg/day for first 6 months. After induction therapy, both groups received EC-MPS 720 mg/day until the end of study at 12 months.
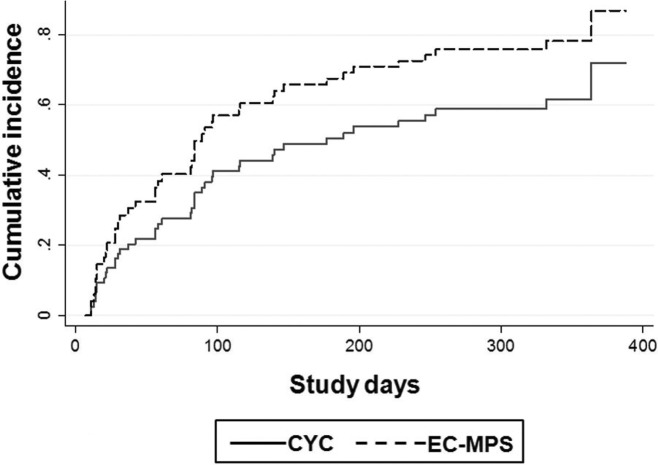
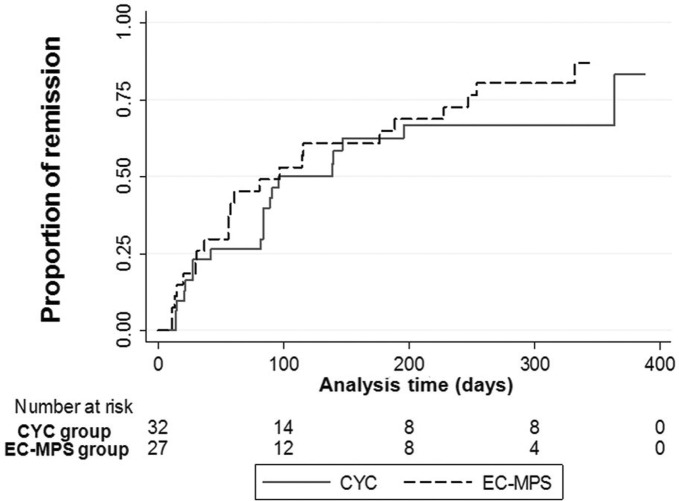
The study was prematurely terminated due to high rate of serious adverse events in CYC arm. Death and serious infections were observed more in the CYC group (15.6% in CYC and 3.5% in EC-MPS; p=0.04). The early discontinuation rates, mainly from serious infections, were significantly higher in CYC group (percentage differences of 16.9; 95% CI 1.3 to 32.4). At the 12th month, both arms were comparable in terms of complete and partial remission rates (68% CYC and 71% EC-MPS) and times to remission (96 days CYC and 97 days EC-MPS). Composites of unfavourable outcomes (death, doubling of serum creatinine, non-remission and intolerance to treatment) were 46.9% and 37% in CYC and EC-MPS (risk difference=9.84; p=0.44).
EC-MPS may have comparable efficacy, but was better tolerated than CYC. EC-MPS should be an alternative choice of treatment for difficult-to-treat LN, particularly in CYC-experienced LN patients. Due to an early termination of the study, further clinical implementation could be cautiously used.
Clinicaltrials.gov ID#NCT01015456.
复发或耐药性狼疮性肾炎(LN)的最佳治疗方法仍不清楚。霉酚酸酯可能是一种避免环磷酰胺(CYC)毒性的替代治疗方法。本研究旨在比较肠溶性吗替麦考酚酯钠(EC-MPS)与静脉注射 CYC 作为诱导治疗。
这是一项为期 12 个月的多中心、开放性、随机对照临床试验。共有 59 例复发(36%)或对先前 CYC 治疗耐药(64%)且活检证实为 III/IV 级的患者被随机分为 CYC(n=32)和 EC-MPS 组(n=27)。CYC 组给予静脉注射 CYC 0.5-1 g/m2 每月一次,EC-MPS 组在最初 6 个月给予 EC-MPS 1440mg/天。诱导治疗后,两组均给予 EC-MPS 720mg/天,持续至 12 个月的研究结束。
由于 CYC 组严重不良事件发生率较高,该研究提前终止。CYC 组观察到更多的死亡和严重感染(CYC 组 15.6%,EC-MPS 组 3.5%;p=0.04)。CYC 组的早期停药率(主要是由于严重感染)明显更高(差异百分比为 16.9%;95%CI 1.3%至 32.4%)。在第 12 个月时,两组在完全和部分缓解率(CYC 组 68%和 EC-MPS 组 71%)和缓解时间(CYC 组 96 天和 EC-MPS 组 97 天)方面相似。不良结局(死亡、血清肌酐加倍、未缓解和不耐受治疗)的复合发生率在 CYC 和 EC-MPS 组分别为 46.9%和 37%(风险差异为 9.84%;p=0.44)。
EC-MPS 可能具有相当的疗效,但耐受性优于 CYC。EC-MPS 应成为治疗难治性 LN 的替代选择,特别是在 CYC 经验丰富的 LN 患者中。由于该研究提前终止,进一步的临床应用需谨慎。
Clinicaltrials.gov ID#NCT01015456。