Ahmad Tariq, Desai Nihar, Wilson Francis, Schulte Phillip, Dunning Allison, Jacoby Daniel, Allen Larry, Fiuzat Mona, Rogers Joseph, Felker G Michael, O'Connor Christopher, Patel Chetan B
Section of Cardiovascular Medicine, Department of Internal Medicine, Yale University School of Medicine, New Haven, Connecticut, United States of America.
Program for Translational Medicine, Yale University School of Medicine, New Haven, Connecticut, United States of America.
PLoS One. 2016 Feb 3;11(2):e0145881. doi: 10.1371/journal.pone.0145881. eCollection 2016.
Classification of acute decompensated heart failure (ADHF) is based on subjective criteria that crudely capture disease heterogeneity. Improved phenotyping of the syndrome may help improve therapeutic strategies.
To derive cluster analysis-based groupings for patients hospitalized with ADHF, and compare their prognostic performance to hemodynamic classifications derived at the bedside.
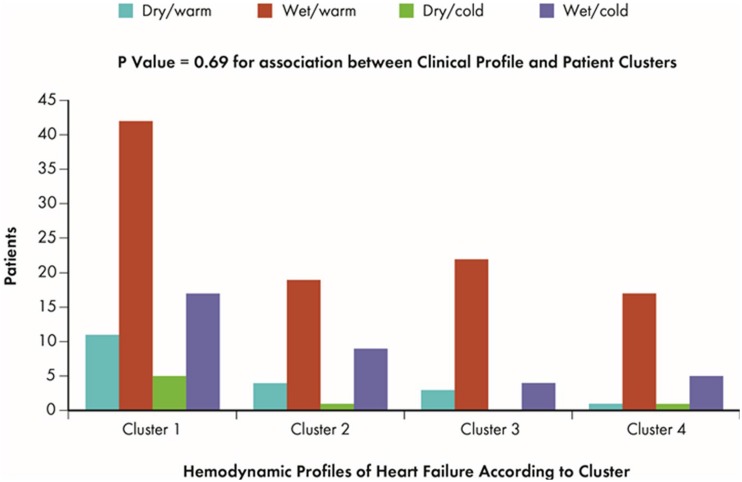
We performed a cluster analysis on baseline clinical variables and PAC measurements of 172 ADHF patients from the ESCAPE trial. Employing regression techniques, we examined associations between clusters and clinically determined hemodynamic profiles (warm/cold/wet/dry). We assessed association with clinical outcomes using Cox proportional hazards models. Likelihood ratio tests were used to compare the prognostic value of cluster data to that of hemodynamic data.
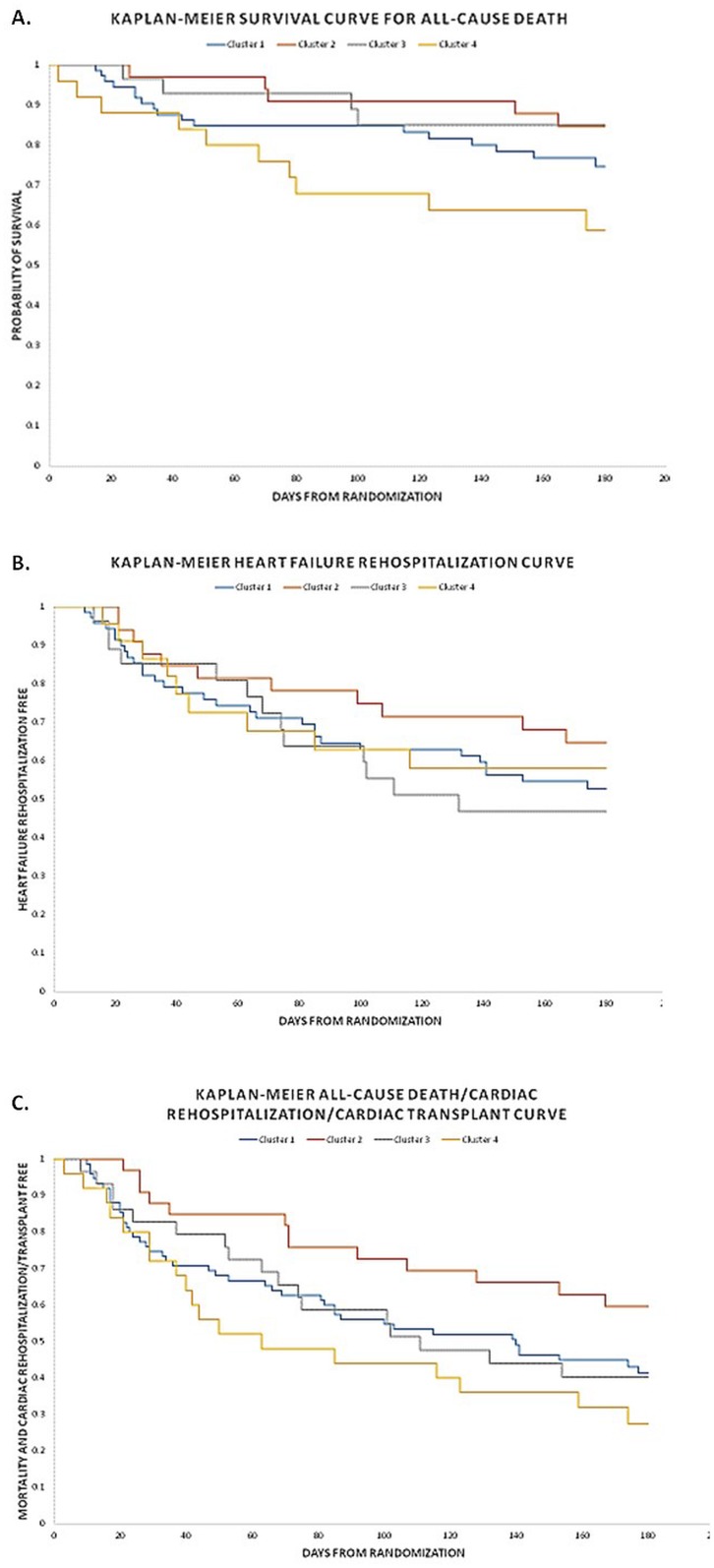
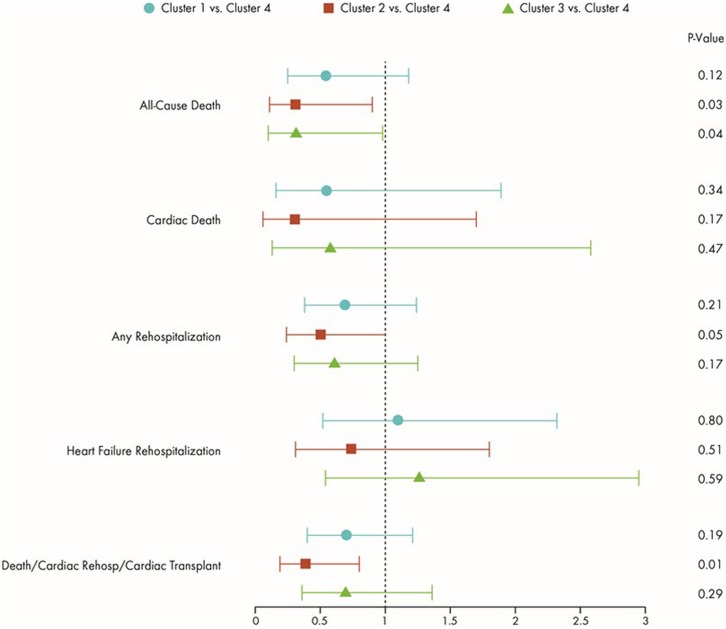
We identified four advanced HF clusters: 1) male Caucasians with ischemic cardiomyopathy, multiple comorbidities, lowest B-type natriuretic peptide (BNP) levels; 2) females with non-ischemic cardiomyopathy, few comorbidities, most favorable hemodynamics; 3) young African American males with non-ischemic cardiomyopathy, most adverse hemodynamics, advanced disease; and 4) older Caucasians with ischemic cardiomyopathy, concomitant renal insufficiency, highest BNP levels. There was no association between clusters and bedside-derived hemodynamic profiles (p = 0.70). For all adverse clinical outcomes, Cluster 4 had the highest risk, and Cluster 2, the lowest. Compared to Cluster 4, Clusters 1-3 had 45-70% lower risk of all-cause mortality. Clusters were significantly associated with clinical outcomes, whereas hemodynamic profiles were not.
By clustering patients with similar objective variables, we identified four clinically relevant phenotypes of ADHF patients, with no discernable relationship to hemodynamic profiles, but distinct associations with adverse outcomes. Our analysis suggests that ADHF classification using simultaneous considerations of etiology, comorbid conditions, and biomarker levels, may be superior to bedside classifications.
急性失代偿性心力衰竭(ADHF)的分类基于主观标准,这些标准粗略地反映了疾病的异质性。对该综合征进行更好的表型分析可能有助于改进治疗策略。
为因ADHF住院的患者得出基于聚类分析的分组,并将其预后表现与床边得出的血流动力学分类进行比较。
我们对来自ESCAPE试验的172例ADHF患者的基线临床变量和肺动脉导管测量值进行了聚类分析。采用回归技术,我们研究了聚类与临床确定的血流动力学特征(暖/冷/湿/干)之间的关联。我们使用Cox比例风险模型评估与临床结局的关联。似然比检验用于比较聚类数据与血流动力学数据的预后价值。
我们确定了四个晚期心力衰竭聚类:1)患有缺血性心肌病、多种合并症、B型利钠肽(BNP)水平最低的男性白种人;2)患有非缺血性心肌病、合并症少、血流动力学最有利的女性;3)患有非缺血性心肌病、血流动力学最不利、疾病晚期的年轻非洲裔美国男性;4)患有缺血性心肌病、伴有肾功能不全、BNP水平最高的老年白种人。聚类与床边得出的血流动力学特征之间无关联(p = 0.70)。对于所有不良临床结局,聚类4风险最高,聚类2风险最低。与聚类4相比,聚类1至3的全因死亡率风险低45 - 70%。聚类与临床结局显著相关,而血流动力学特征则不然。
通过对具有相似客观变量的患者进行聚类,我们确定了ADHF患者的四种临床相关表型,它们与血流动力学特征无明显关系,但与不良结局有明显关联。我们的分析表明,同时考虑病因、合并症情况和生物标志物水平的ADHF分类可能优于床边分类。