Schwinger Catherine, Fadnes Lars T, Van den Broeck Jan
Center for International Health, Department of Global Public Health and Primary Care, and
Center for International Health, Department of Global Public Health and Primary Care, and Department of Clinical Dentistry, University of Bergen, Bergen, Norway.
Am J Clin Nutr. 2016 Mar;103(3):801-7. doi: 10.3945/ajcn.115.118679. Epub 2016 Feb 3.
Growth assessment based on the WHO child growth velocity standards can potentially be used to predict adverse health outcomes. Nevertheless, there are very few studies on growth velocity to predict mortality.
We aimed to determine the ability of various growth velocity measures to predict child death within 3 mo and to compare it with those of attained growth measures.
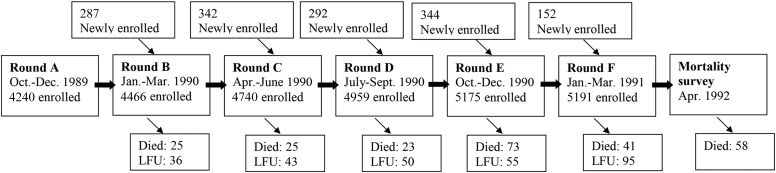
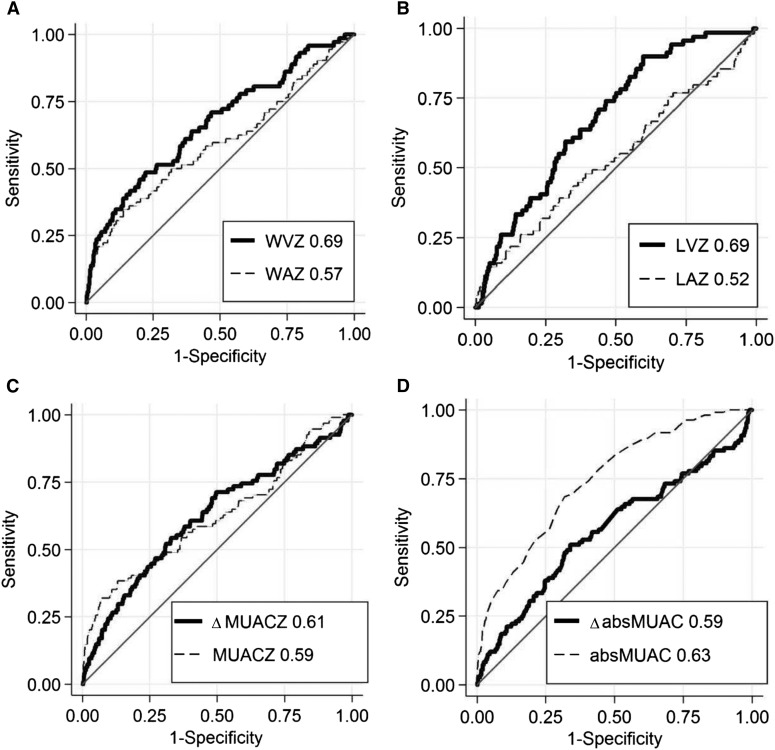
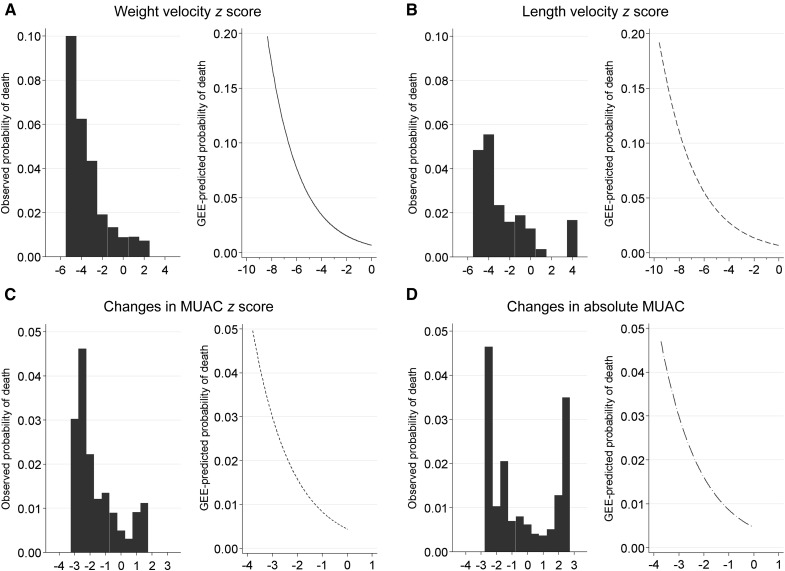
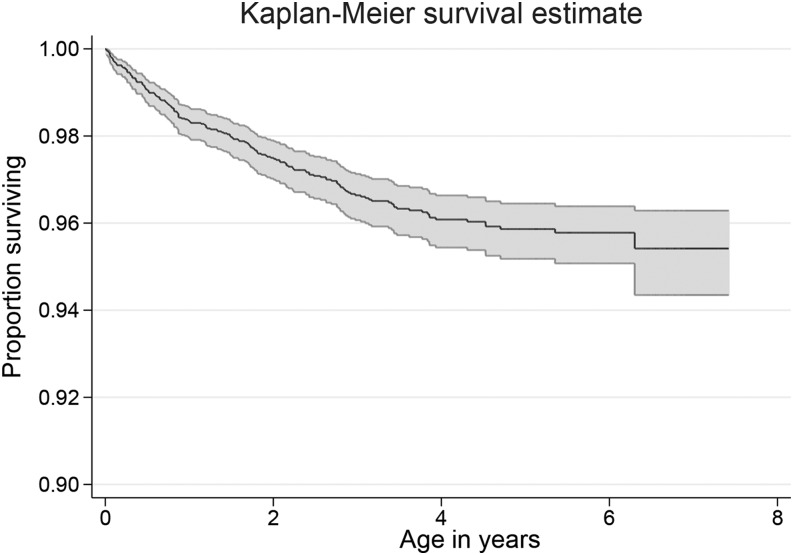
Data from 5657 children <5 y old who were enrolled in a cohort study in the Democratic Republic of Congo were used. Children were measured up to 6 times in 3-mo intervals, and 246 (4.3%) children died during the study period. Generalized estimating equation (GEE) models informed the mortality risk within 3 mo for weight and length velocity z scores and 3-mo changes in midupper arm circumference (MUAC). We used receiver operating characteristic (ROC) curves to present balance in sensitivity and specificity to predict child death.
GEE models showed that children had an exponential increase in the risk of dying with decreasing growth velocity in all 4 indexes (1.2- to 2.4-fold for every unit decrease). A length and weight velocity z score of <-3 was associated with an 11.8- and a 7.9-fold increase, respectively, in the RR of death in the subsequent 3-mo period (95% CIs: 3.9, 35.5, and 3.9, 16.2, respectively). Weight and length velocity z scores had better predictive abilities [area under the ROC curves (AUCs) of 0.67 and 0.69] than did weight-for-age (AUC: 0.57) and length-for-age (AUC: 0.52) z scores. Among wasted children (weight-for-height z score <-2), the AUC of weight velocity z scores was 0.87. Absolute MUAC performed best among the attained indexes (AUC: 0.63), but longitudinal assessment of MUAC-based indexes did not increase the predictive value.
Although repeated growth measures are slightly more complex to implement, their superiority in mortality-predictive abilities suggests that these could be used more for identifying children at increased risk of death.
基于世界卫生组织儿童生长速度标准的生长评估有可能用于预测不良健康结局。然而,关于生长速度预测死亡率的研究非常少。
我们旨在确定各种生长速度测量方法预测3个月内儿童死亡的能力,并将其与已获得的生长测量方法进行比较。
使用了刚果民主共和国一项队列研究中5657名5岁以下儿童的数据。儿童每隔3个月测量一次,最多测量6次,246名(4.3%)儿童在研究期间死亡。广义估计方程(GEE)模型用于计算体重和身长速度z评分以及上臂中部周长(MUAC)3个月变化的3个月内死亡风险。我们使用受试者工作特征(ROC)曲线来展示预测儿童死亡时敏感性和特异性的平衡。
GEE模型显示,在所有4项指标中,随着生长速度降低,儿童死亡风险呈指数级增加(每降低一个单位增加1.2至2.4倍)。身长和体重速度z评分<-3分别与随后3个月内死亡风险增加11.8倍和7.9倍相关(95%置信区间分别为3.9、35.5和3.9、16.2)。体重和身长速度z评分的预测能力[ROC曲线下面积(AUC)分别为0.67和0.69]优于年龄别体重(AUC:0.57)和年龄别身长(AUC:0.52)z评分。在消瘦儿童(身高别体重z评分<-2)中,体重速度z评分的AUC为0.87。在已获得的指标中,绝对MUAC表现最佳(AUC:0.63),但基于MUAC指标的纵向评估并未增加预测价值。
尽管重复生长测量的实施略显复杂,但其在死亡率预测能力方面的优势表明,这些测量方法可更多地用于识别死亡风险增加的儿童。