Choi Seung Woo, Lee Jae Yeun, Lew Helen
Department of Ophthalmology, Bundang CHA Medical Center, CHA University, Seongnam, Korea.
Korean J Ophthalmol. 2016 Feb;30(1):1-9. doi: 10.3341/kjo.2016.30.1.1. Epub 2016 Jan 21.
To evaluate the efficacy and safety of customized orbital decompression surgery combined with eyelid surgery or strabismus surgery for mild to moderate thyroid-associated ophthalmopathy (TAO).
Twenty-seven consecutive subjects who were treated surgically for proptosis with disfigurement or diplopia after medical therapy from September 2009 to July 2012 were included in the analysis. Customized orbital decompression surgery with correction of eyelid retraction and extraocular movement disorders was simultaneously performed. The patients had a minimum preoperative period of 3 months of stable range of ocular motility and eyelid position. All patients had inactive TAO and were euthyroid at the time of operation. Preoperative and postoperative examinations, including vision, margin reflex distance, Hertel exophthalmometry, ocular motility, visual fields, Goldmann perimetry, and subject assessment of the procedure, were performed in all patients. Data were analyzed using paired t-test (PASW Statistics ver. 18.0).
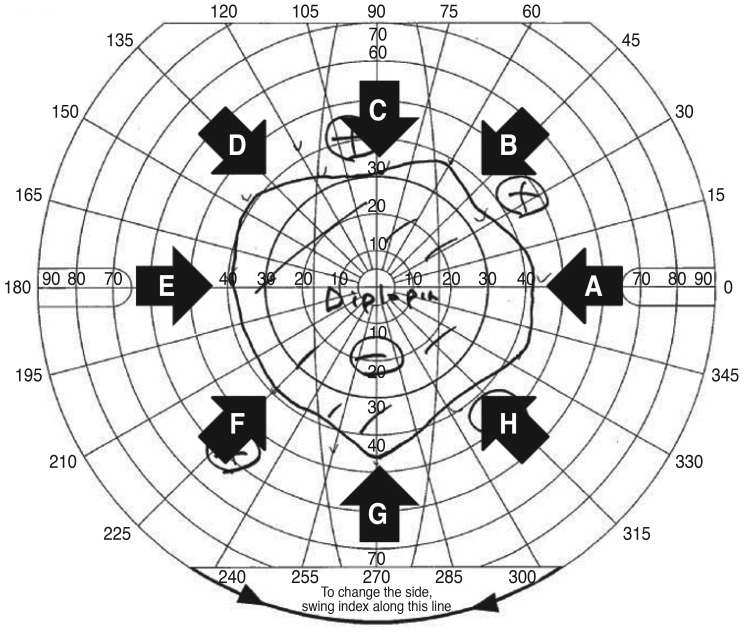
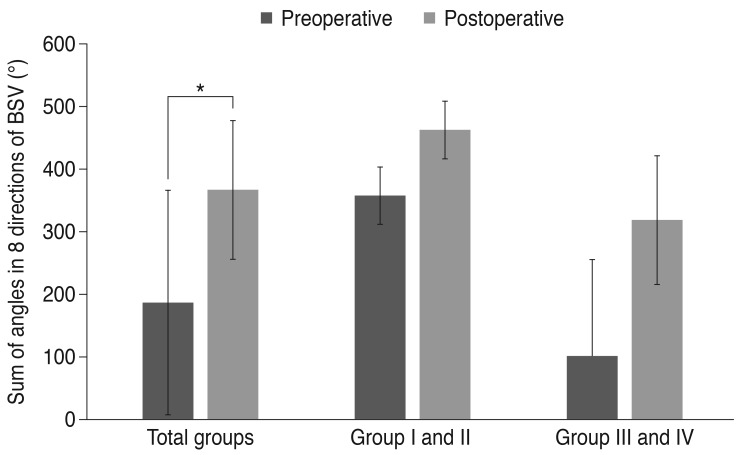
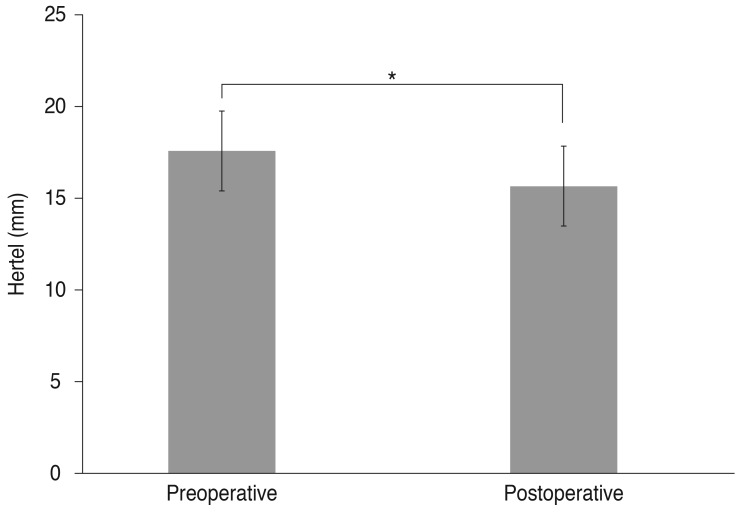
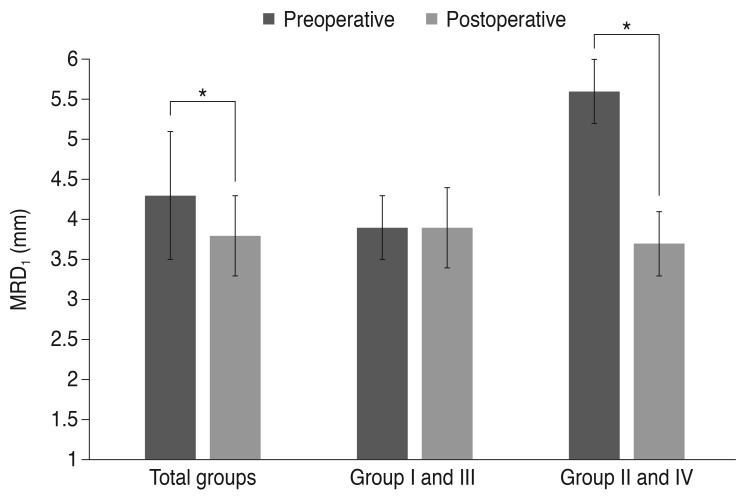
Forty-nine decompressions were performed on 27 subjects (16 females, 11 males; mean age, 36.6 ± 11.6 years). Twenty-two patients underwent bilateral operations; five required only unilateral orbital decompression. An average proptosis of 15.6 ± 2.2 mm (p = 0.00) was achieved, with a mean preoperative Hertel measurement of 17.6 ± 2.2 mm. Ocular motility was corrected through recession of the extraocular muscle in three cases, and no new-onset diplopia or aggravated diplopia was noted. The binocular single vision field increased in all patients. Eyelid retraction correction surgery was simultaneously performed in the same surgical session in 10 of 49 cases, and strabismus and eyelid retraction surgery were performed in the same surgical session in two cases. Margin reflex distance decreased from a preoperative average of 4.3 ± 0.8 to 3.8 ± 0.5 mm postoperatively.
The customized orbital decompression procedure decreased proptosis and improved diplopia, in a range comparable to those achieved through more stepwise techniques, and had favorable cosmetic results when combined with eyelid surgery or strabismus surgery for mild to moderate TAO.
评估定制眼眶减压手术联合眼睑手术或斜视手术治疗轻至中度甲状腺相关眼病(TAO)的疗效和安全性。
分析2009年9月至2012年7月期间连续27例经药物治疗后因眼球突出伴毁容或复视而接受手术治疗的患者。同时进行定制眼眶减压手术并矫正眼睑退缩和眼球运动障碍。患者术前眼球运动范围和眼睑位置稳定至少3个月。所有患者的TAO均处于静止期,且手术时甲状腺功能正常。对所有患者进行术前和术后检查,包括视力、边缘反射距离、Hertel突眼计测量、眼球运动、视野、Goldmann视野计检查以及患者对手术的评估。使用配对t检验(PASW Statistics 18.0版)进行数据分析。
对27例患者(16例女性,11例男性;平均年龄36.6±11.6岁)进行了49次减压手术。22例患者接受双侧手术;5例仅需单侧眼眶减压。平均突眼度降低了15.6±2.2 mm(p = 0.00),术前平均Hertel测量值为17.6±2.2 mm。3例患者通过眼外肌后徙矫正了眼球运动,未发现新发复视或复视加重。所有患者的双眼单视野均增加。49例手术中有10例在同一手术中同时进行了眼睑退缩矫正手术,2例在同一手术中进行了斜视和眼睑退缩手术。边缘反射距离从术前平均4.3±0.8 mm降至术后3.8±0.