Feng Yanfang, Hodiamont Caspar J, van Hest Reinier M, Brul Stanley, Schultsz Constance, Ter Kuile Benno H
Department of Molecular Biology and Microbial Food Safety, Swammerdam Institute of Life Sciences, University of Amsterdam, Amsterdam, The Netherlands.
Department of Medical Microbiology, Academic Medical Center, Amsterdam, the Netherlands.
PLoS One. 2016 Feb 12;11(2):e0149310. doi: 10.1371/journal.pone.0149310. eCollection 2016.
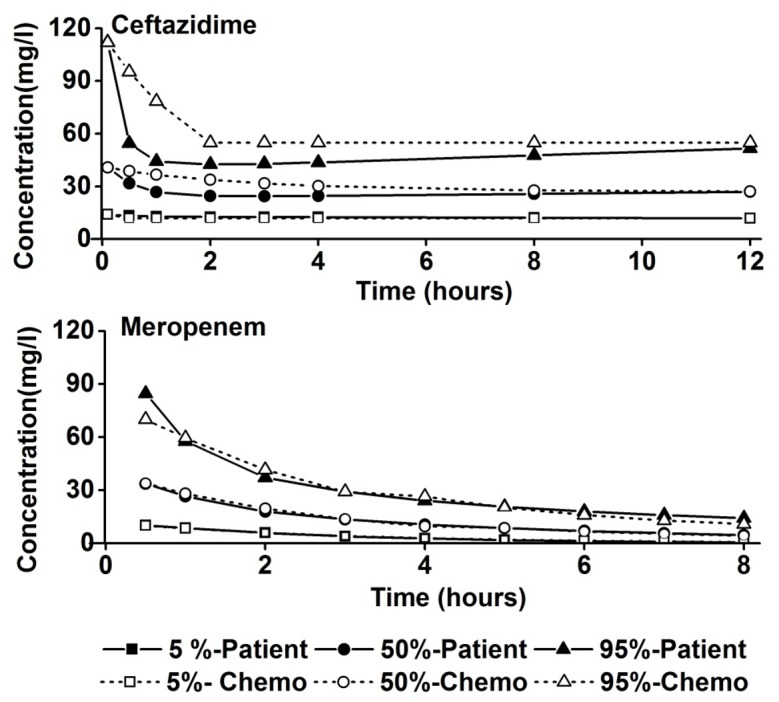
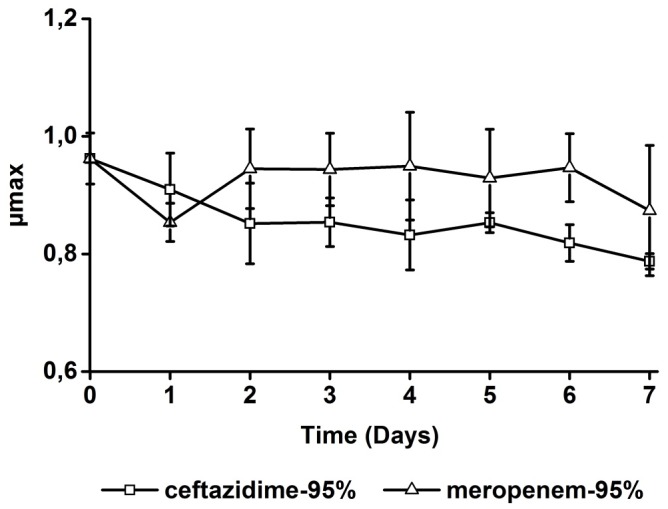
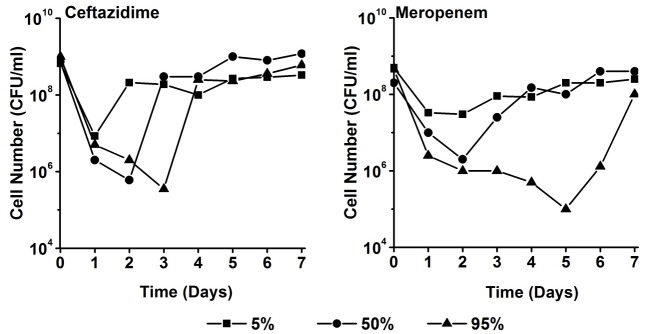
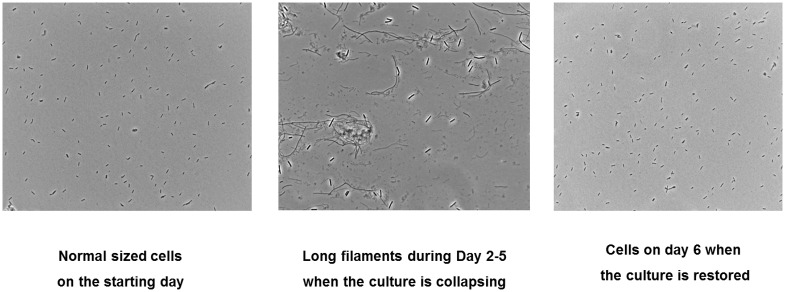
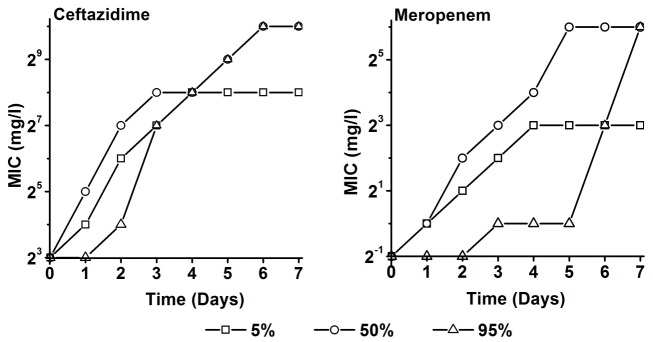
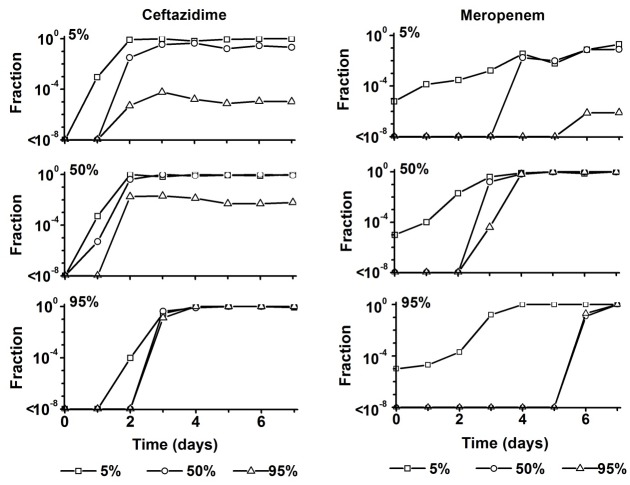
During treatment of infections with antibiotics in critically ill patients in the intensive care resistance often develops. This study aims to establish whether under those conditions this resistance can develop de novo or that genetic exchange between bacteria is by necessity involved. Chemostat cultures of Pseudomonas aeruginosa were exposed to treatment regimes with ceftazidime and meropenem that simulated conditions expected in patient plasma. Development of antibiotic resistance was monitored and mutations in resistance genes were searched for by sequencing PCR products. Even at the highest concentrations that can be expected in patients, sufficient bacteria survived in clumps of filamentous cells to recover and grow out after 3 to 5 days. At the end of a 7 days simulated treatment, the minimal inhibitory concentration (MIC) had increased by a factor between 10 and 10,000 depending on the antibiotic and the treatment protocol. The fitness costs of resistance were minimal. In the resistant strains, only three mutations were observed in genes associated with beta-lactam resistance. The development of resistance often observed during patient treatment can be explained by de novo acquisition of resistance and genetic exchange of resistance genes is not by necessity involved. As far as conclusions based on an in vitro study using P. aeruginosa and only two antibiotics can be generalized, it seems that development of resistance can be minimized by treating with antibiotics in the highest concentration the patient can endure for the shortest time needed to eliminate the infection.
在重症监护病房中,危重症患者使用抗生素治疗感染时,耐药性常常会出现。本研究旨在确定在这些情况下,这种耐药性是会重新产生,还是必然涉及细菌之间的基因交换。将铜绿假单胞菌的恒化器培养物暴露于头孢他啶和美罗培南的治疗方案下,这些方案模拟了患者血浆中预期的情况。监测抗生素耐药性的发展,并通过对聚合酶链反应(PCR)产物进行测序来寻找耐药基因中的突变。即使在患者可能达到的最高浓度下,丝状细胞团中仍有足够的细菌存活下来,并在3至5天后复苏并生长。在7天的模拟治疗结束时,根据抗生素和治疗方案的不同,最低抑菌浓度(MIC)增加了10至10000倍。耐药性的适应性代价极小。在耐药菌株中,与β-内酰胺耐药性相关的基因中仅观察到三个突变。患者治疗期间经常观察到的耐药性发展可以通过耐药性的重新获得来解释,并不必然涉及耐药基因的基因交换。就基于使用铜绿假单胞菌和仅两种抗生素的体外研究得出的结论而言,如果可以推广的话,似乎通过以患者能够耐受的最高浓度、在消除感染所需的最短时间内使用抗生素进行治疗,可以将耐药性的发展降至最低。