Schranz Dietmar, Voelkel Norbert F
Pediatric Heart Center, Justus-Liebig University Clinic, Feulgenstr. 12, 30385, Giessen, Germany.
School of Pharmacy, Virginia Commonwealth University, Richmond, VA, USA.
Eur J Pediatr. 2016 Apr;175(4):445-55. doi: 10.1007/s00431-016-2700-3. Epub 2016 Feb 19.
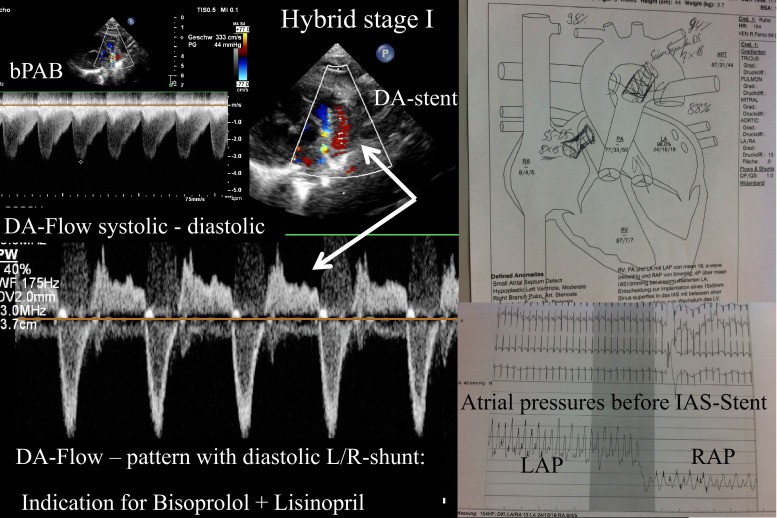
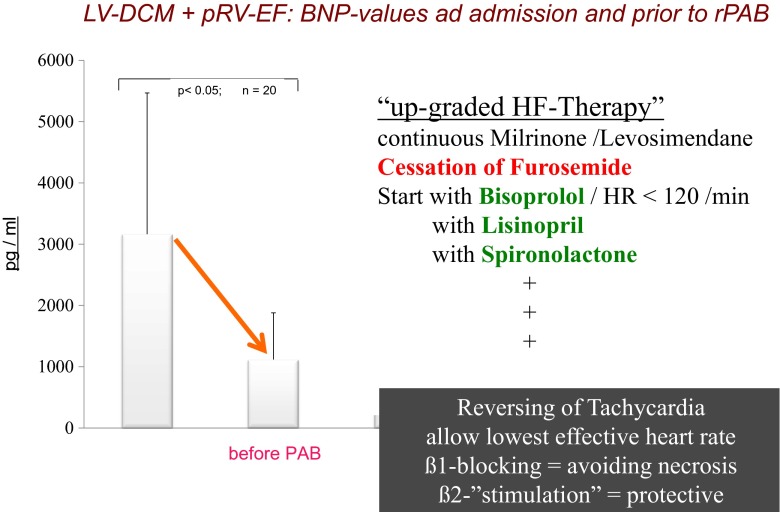
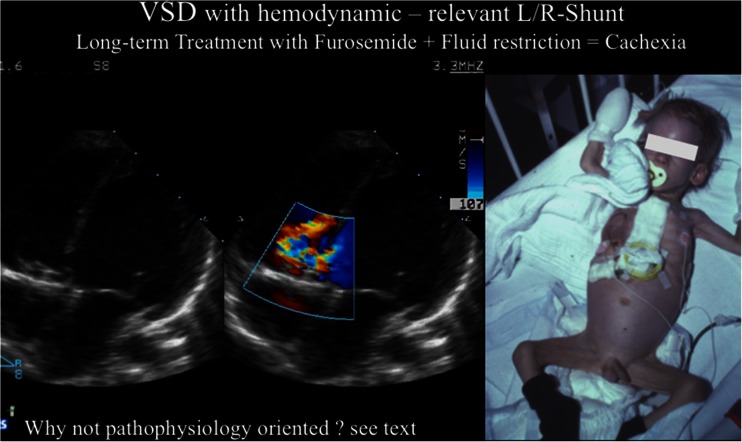
Major advances in chronic heart failure (cHF) therapy have been achieved and documented in adult patients, while research regarding the mechanisms and therapy of cHF in children has lagged behind. Based on receptor physiological studies and pharmacological knowledge, treatment with specific ß1-adrenergic receptor blocker (ARB), tissue angiotensin-converting enzyme inhibitor (ACE-I), and mineralocorticoid antagonists have to be recommended in children despite lack of sufficient data derived from prospective randomized studies. At our institution, bisoprolol, lisinopril, and spironolactone have been firmly established to treat systolic cHF, hypoplastic left heart syndrome (HLHS) following hybrid approach and congenital left-right shunt diseases, latest in patients where surgery has to be delayed. Chronic therapy with long-acting diuretics and fluid restriction are not advocated because short-term effects are achieved at the expense of further neuro-humoral stimulation. It remains unclear why diuretics are recommended although evidence-based studies, documenting long-term benefit, are missing. However, that is true for all currently used drugs for pediatric cHF.
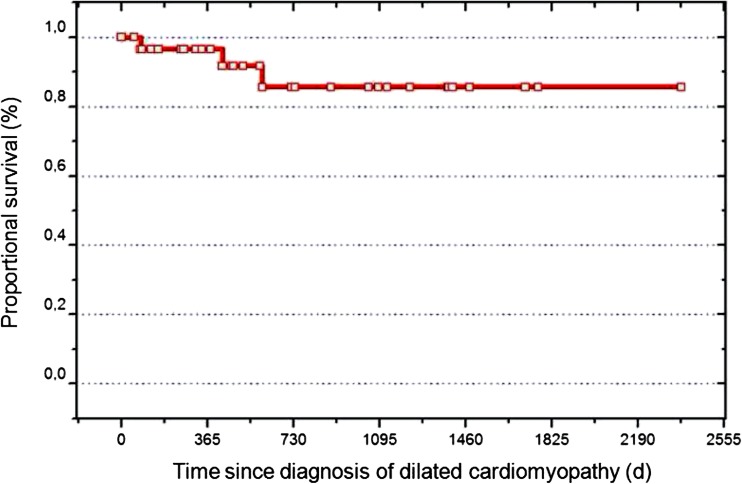
This review focuses on the prevailing "nihilism" of cHF therapy in children with the goal to encourage physicians to treat pediatric cHF with a rationally designed therapy, which combines available agents that have been shown to improve survival in adult patients with cHF. Because of the lack of clinical trials, which generate the needed evidence, surrogate variables like heart and respiratory rate, weight gain, image-derived data, and biomarkers should be monitored and used instead. The recommended pharmacological therapy for systolic heart failure is also provided as the basis for utilizing reversible pulmonary arterial banding (PAB) as a novel strategy in young children with dilative cardiomyopathy (DCM) with preserved right ventricular function.
• Heart failure (HF) in children is a serious public health concern. • HF has numerous etiologies, but unspecific symptoms. • HF interplays among neuro-humoral, and molecular abnormalities. • Pediatric cHF-therapy is currently based on loop-diuretics, fluid restriction and digoxin. What is New: • Cardiac function analysis has to include cardiac synchrony and VVI. • Considering enormous potential of cardiac regeneration, therapy has to extend with selective ß1-ARB, tissue ACE-I and mineralocorticoid blockers, loop-diuretics avoided as ever possible. • Inhibition of the endogenous neuro-humoral stimulation is monitored by surrogate parameters as heart and breath rate and systolic and diastolic blood pressure. • Advocated HF therapy serves for regenerative strategies as reversible Pulmonary Artery Banding in DCM.
慢性心力衰竭(cHF)治疗在成年患者中已取得重大进展并有文献记载,而关于儿童cHF的发病机制和治疗的研究却滞后了。基于受体生理学研究和药理学知识,尽管缺乏前瞻性随机研究的充分数据,但仍建议在儿童中使用特定的β1 - 肾上腺素能受体阻滞剂(ARB)、组织血管紧张素转换酶抑制剂(ACE - I)和盐皮质激素拮抗剂进行治疗。在我们机构,比索洛尔、赖诺普利和螺内酯已被确定用于治疗收缩性cHF、经混合治疗后的左心发育不全综合征(HLHS)以及先天性左右分流疾病,最近也用于手术不得不推迟的患者。不主张长期使用利尿剂和限制液体摄入进行慢性治疗,因为短期效果是以进一步刺激神经 - 体液为代价实现的。尽管缺乏记录长期益处的循证研究,但仍推荐使用利尿剂,原因尚不清楚。然而,目前所有用于小儿cHF的药物都是如此。
本综述聚焦于儿童cHF治疗中普遍存在的“虚无主义”,目的是鼓励医生采用合理设计的疗法治疗小儿cHF,该疗法结合已证明能提高成年cHF患者生存率的现有药物。由于缺乏产生所需证据的临床试验,应监测并使用诸如心率和呼吸频率、体重增加、影像数据和生物标志物等替代变量。还提供了收缩性心力衰竭的推荐药物治疗方法,作为在右心室功能保留的扩张型心肌病(DCM)幼儿中采用可逆性肺动脉环扎术(PAB)这一新型策略的基础。
• 儿童心力衰竭(HF)是一个严重的公共卫生问题。• HF有多种病因,但症状不具特异性。• HF在神经 - 体液和分子异常之间相互作用。• 小儿cHF治疗目前基于襻利尿剂、液体限制和地高辛。新内容:• 心功能分析必须包括心脏同步性和VVI。• 考虑到心脏再生的巨大潜力,治疗必须扩展到选择性β1 - ARB、组织ACE - I和盐皮质激素阻滞剂,尽可能避免使用襻利尿剂。• 通过心率和呼吸频率以及收缩压和舒张压等替代参数监测内源性神经 - 体液刺激的抑制情况。• 推荐的HF治疗方法可用于再生策略,如DCM中的可逆性肺动脉环扎术。