Liu Haisong, Andrews David W, Evans James J, Werner-Wasik Maria, Yu Yan, Dicker Adam Paul, Shi Wenyin
Department of Radiation Oncology, Thomas Jefferson University , Philadelphia, PA , USA.
Department of Neurological Surgery, Thomas Jefferson University , Philadelphia, PA , USA.
Front Oncol. 2016 Feb 11;6:26. doi: 10.3389/fonc.2016.00026. eCollection 2016.
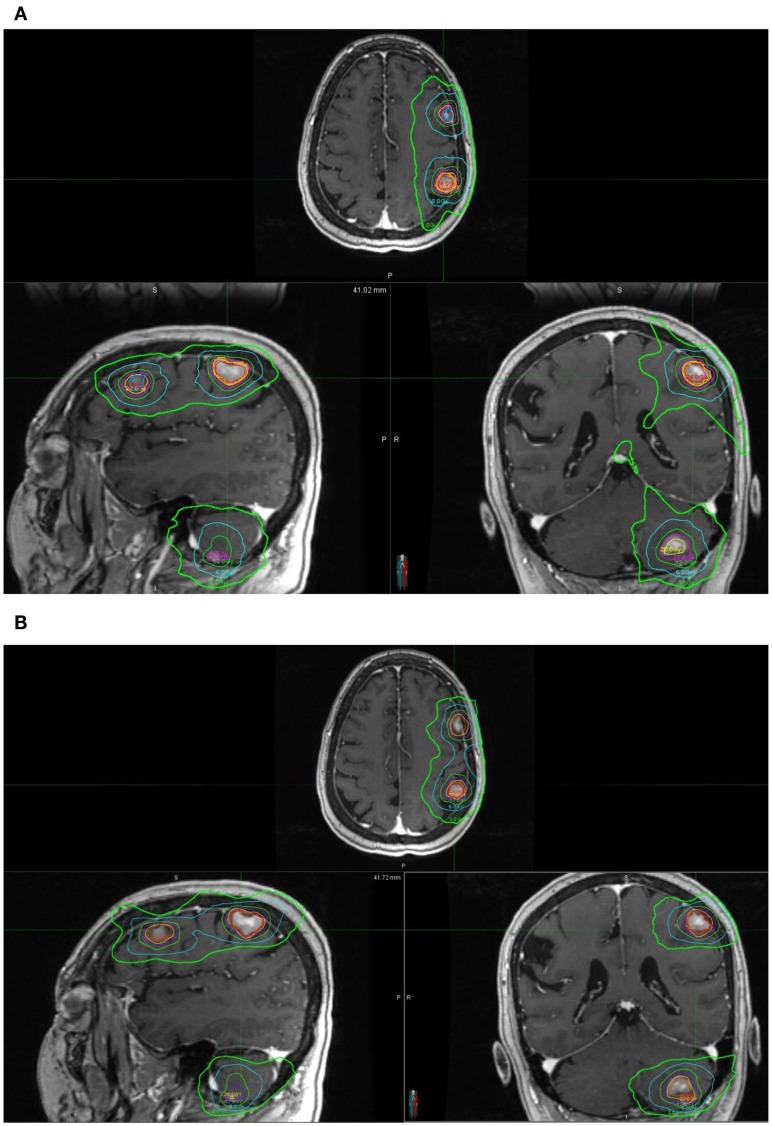
This study compares the dosimetry and efficiency of two modern radiosurgery [stereotactic radiosurgery (SRS)] modalities for multiple brain metastases [Gamma Knife (GK) and LINAC-based RapidArc/volumetric modulated arc therapy], with a special focus on the comparison of low-dose spread.
Six patients with three or four small brain metastases were used in this study. The size of targets varied from 0.1 to 10.5 cc. SRS doses were prescribed according to the size of lesions. SRS plans were made using both Gamma Knife(®) Perfexion and a single-isocenter, multiple non-coplanar RapidArc(®). Dosimetric parameters analyzed included RTOG conformity index (CI), gradient index (GI), 12 Gy isodose volume (V 12Gy) for each target, and the dose "spread" (Dspread) for each plan. Dspread reflects SRS plan's capability of confining radiation to within the local vicinity of the lesion and to not spread out to the surrounding normal brain tissues. Each plan has a dose (Dspread), such that once dose decreases below Dspread (on total tissue dose-volume histogram), isodose volume starts increasing dramatically. Dspread is defined as that dose when volume increase first exceeds 20 cc/0.1 Gy dose decrease.
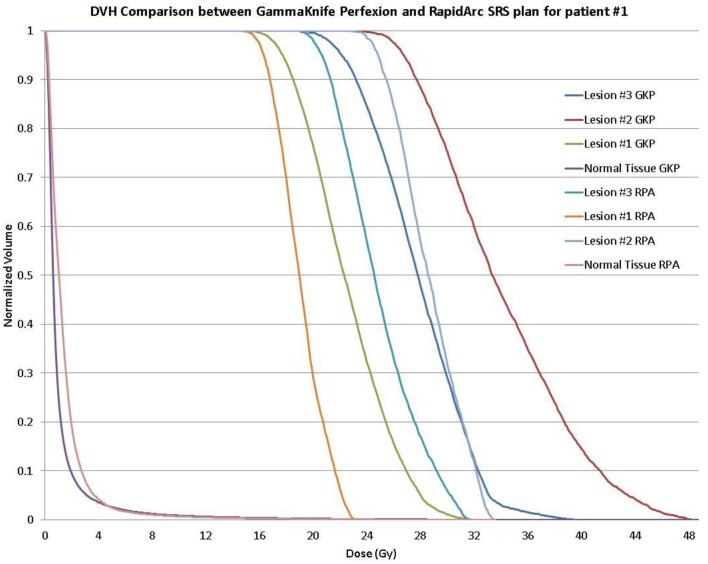
RapidArc SRS has smaller CI (1.19 ± 0.14 vs. 1.50 ± 0.16, p < 0.001) and larger GI (4.77 ± 1.49 vs. 3.65 ± 0.98, p < 0.01). V 12Gy results were comparable (2.73 ± 1.38 vs. 3.06 ± 2.20 cc, p = 0.58). Moderate to lower dose spread, V6, V4.5, and V3, were also equivalent. GK plans achieved better very low-dose spread (≤3 Gy) and also had slightly smaller Dspread, 1.9 vs. 2.5 Gy. Total treatment time for GK is estimated between 60 and 100 min. GK treatments are between 3 and 5 times longer compared to RapidArc treatment techniques.
Dosimetric parameters reflecting prescription dose conformality (CI), dose fall off (GI), radiation necrosis indicator (V 12Gy), and dose spread (Dspread) were compared between GK SRS and RapidArc SRS for multi-mets. RapidArc plans have smaller CI but larger GI. V 12Gy are comparable. GK appears better at reducing only very low-dose spread (<3 Gy). The treatment time of RapidArc SRS is significantly reduced compared to GK SRS.
本研究比较两种现代放射外科[立体定向放射外科(SRS)]治疗多发脑转移瘤的剂量学和效率[伽玛刀(GK)和基于直线加速器的容积弧形调强放疗(RapidArc)],特别关注低剂量分布的比较。
本研究纳入6例有3个或4个小脑转移瘤的患者。靶区大小从0.1到10.5立方厘米不等。根据病变大小规定SRS剂量。使用伽玛刀(®)Perfexion和单等中心、多个非共面容积弧形调强放疗(RapidArc)(®)制定SRS计划。分析的剂量学参数包括美国放射肿瘤学会(RTOG)适形指数(CI)、梯度指数(GI)、每个靶区的12 Gy等剂量体积(V12Gy)以及每个计划的剂量“分布”(Dspread)。Dspread反映SRS计划将辐射局限于病变局部附近且不扩散到周围正常脑组织的能力。每个计划都有一个剂量(Dspread),即一旦剂量在总组织剂量 - 体积直方图上降至Dspread以下,等剂量体积就会开始急剧增加。Dspread定义为体积增加首次超过20立方厘米/0.1 Gy剂量降低时的剂量。
容积弧形调强放疗(RapidArc)SRS的CI较小(1.19±0.14对1.50±0.16,p<0.001),GI较大(4.77±1.49对3.65±0.98,p<0.01)。V12Gy结果相当(2.73±1.38对3.06±2.20立方厘米,p = 0.58)。中低剂量分布、V6、V4.5和V3也相当。GK计划在极低剂量分布(≤3 Gy)方面表现更好,且Dspread也略小,分别为1.9 Gy和2.5 Gy。GK的总治疗时间估计在60至100分钟之间。与容积弧形调强放疗(RapidArc)治疗技术相比,GK治疗时间长3至5倍。
比较了伽玛刀(GK)SRS和容积弧形调强放疗(RapidArc)SRS在治疗多发转移瘤时反映处方剂量适形性(CI)、剂量下降(GI)、放射性坏死指标(V12Gy)和剂量分布(Dspread)的剂量学参数。容积弧形调强放疗(RapidArc)计划的CI较小但GI较大。V12Gy相当。GK在仅降低极低剂量分布(<3 Gy)方面似乎更好。与伽玛刀(GK)SRS相比,容积弧形调强放疗(RapidArc)SRS的治疗时间显著缩短。