Pierce G L, Harris S A, Seals D R, Casey D P, Barlow P B, Stauss H M
Department of Health and Human Physiology, University of Iowa, Iowa City, IA, USA.
Abboud Cardiovascular Research Center, University of Iowa, Iowa City, IA, USA.
J Hum Hypertens. 2016 Sep;30(9):513-20. doi: 10.1038/jhh.2016.3. Epub 2016 Feb 25.
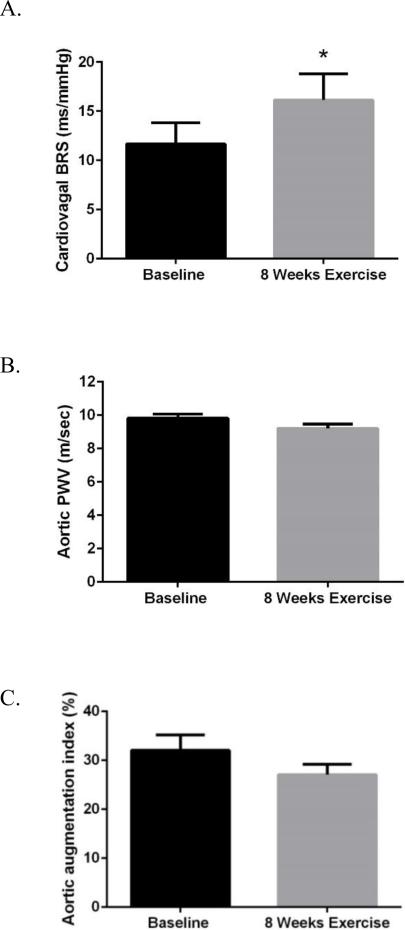
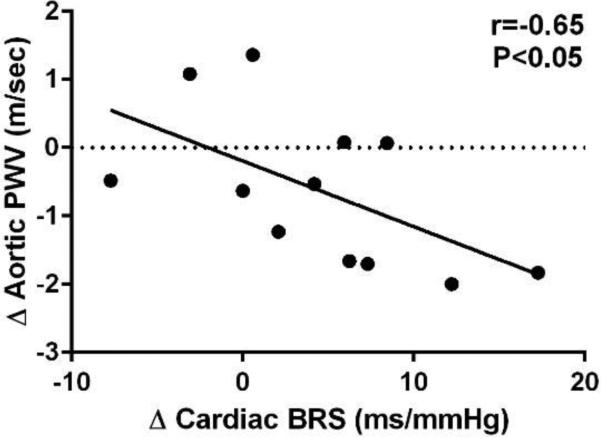
We hypothesised that differences in cardiac baroreflex sensitivity (BRS) would be independently associated with aortic stiffness and augmentation index (AI), clinical biomarkers of cardiovascular disease risk, among young sedentary and middle-aged/older sedentary and endurance-trained adults. A total of 36 healthy middle-aged/older (age 55-76 years, n=22 sedentary and n=14 endurance-trained) and 5 young sedentary (age 18-31 years) adults were included in a cross-sectional study. A subset of the middle-aged/older sedentary adults (n=12) completed an 8-week-aerobic exercise intervention. Invasive brachial artery blood pressure waveforms were used to compute spontaneous cardiac BRS (via sequence technique), estimated aortic pulse wave velocity (PWV) and AI (AI, via brachial-aortic transfer function and wave separation analysis). In the cross-sectional study, cardiac BRS was 71% lower in older compared with young sedentary adults (P<0.05), but only 40% lower in older adults who performed habitual endurance exercise (P=0.03). In a regression model that included age, sex, resting heart rate, mean arterial pressure (MAP), body mass index and maximal exercise oxygen uptake, estimated aortic PWV (β±s.e.=-5.76±2.01, P=0.01) was the strongest predictor of BRS (model R(2)=0.59, P<0.001). The 8-week-exercise intervention improved BRS by 38% (P=0.04) and this change in BRS was associated with improved aortic PWV (r=-0.65, P=0.044, adjusted for changes in MAP). Age- and endurance-exercise-related differences in cardiac BRS are independently associated with corresponding alterations in aortic PWV among healthy adults, consistent with a mechanistic link between variations in the sensitivity of the baroreflex and aortic stiffness with age and exercise.
我们假设,在久坐不动的年轻成年人、中年/老年久坐不动的成年人以及耐力训练的成年人中,心脏压力反射敏感性(BRS)的差异会与主动脉僵硬度和增强指数(AI)独立相关,而主动脉僵硬度和增强指数是心血管疾病风险的临床生物标志物。一项横断面研究纳入了总共36名健康的中年/老年(年龄55 - 76岁,22名久坐不动,14名进行耐力训练)和5名久坐不动的年轻(年龄18 - 31岁)成年人。一部分中年/老年久坐不动的成年人(n = 12)完成了为期8周的有氧运动干预。通过侵入性肱动脉血压波形来计算自发性心脏BRS(通过序列技术)、估计主动脉脉搏波速度(PWV)和AI(AI,通过肱动脉 - 主动脉传递函数和波分离分析)。在横断面研究中,与久坐不动的年轻成年人相比,老年人心脏BRS降低了71%(P < 0.05),但在进行习惯性耐力运动的老年人中仅降低了40%(P = 0.03)。在一个包含年龄、性别、静息心率、平均动脉压(MAP)、体重指数和最大运动摄氧量的回归模型中,估计的主动脉PWV(β±标准误=-5.76±2.01,P = 0.01)是BRS的最强预测因子(模型R² = 0.59,P < 0.001)。为期8周的运动干预使BRS提高了38%(P = 0.04),并且BRS的这种变化与主动脉PWV的改善相关(r = -0.65,P = 0.044,经MAP变化调整)。在健康成年人中,与年龄和耐力运动相关的心脏BRS差异与主动脉PWV的相应改变独立相关,这与压力反射敏感性变化和主动脉僵硬度随年龄及运动的机制联系一致。