Costantini Massimo, Rabitti Elisa, Beccaro Monica, Fusco Flavio, Peruselli Carlo, La Ciura Pietro, Valle Alessandro, Suriani Cinzia, Berardi Maria Alejandra, Valenti Danila, Mosso Felicita, Morino Piero, Zaninetta Giovanni, Tubere Giorgio, Piazza Massimo, Sofia Michele, Di Leo Silvia, Higginson Irene J
Palliative Care Unit, Arcispedale Santa Maria Nuova-IRCCS, Reggio Emilia, Italy.
Academy of Sciences of Palliative Medicine, Bentivoglio, Bologna, Italy.
BMC Palliat Care. 2016 Feb 26;15:23. doi: 10.1186/s12904-016-0095-6.
There is an increasing requirement to assess outcomes, but few measures have been tested for advanced medical illness. We aimed to test the validity, reliability and responsiveness of the Palliative care Outcome Scale (POS), and to analyse predictors of change after the transition to palliative care.
Phase 1: multicentre, mixed method study comprising cognitive and qualitative interviews with patients and staff, cultural refinement and adaption. Phase 2: consecutive cancer patients on admission to 8 inpatient hospices and 7 home-based teams were asked to complete the POS, the EORTC QLQ-C15-PAL and the FACIT-Sp (T0), to assess internal consistency, convergent and divergent validity. After 6 days (T1) patients and staff completed the POS to assess responsiveness to change (T1-T0), and agreement between self-assessed POS and POS completed by the staff. Finally, we asked hospices an assessment 24-48 h after T1 to assess its reliability (test re-test analysis).
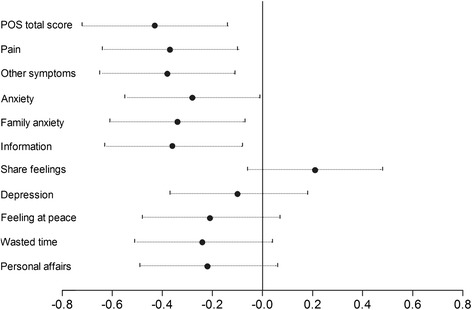
Phase I: 209 completed POS questionnaires and 29 cognitive interviews were assessed, revisions made and one item substituted. Phase II: 295 consecutive patients admitted to 15 PCTs were approached, 175 (59.3 %) were eligible, and 150 (85.7 %) consented. Consent was limited by the severity of illness in 40 % patients. We found good convergent validity, with strong and moderate correlations (r ranged 0.5-0.8) between similar items from the POS, the QLQ-C15-PAL and the FACIT-Sp. As hypothesised, the physical function subscale of QLQ-C15-PAL was not correlated with any POS item (r ranged -0.16-0.02). We found acceptable to good test re-test reliability in both versions for 6 items. We found significant clinical improvements during the first week of palliative care in 7/10 items assessed-pain, other symptoms, patient and family anxiety, information, feeling at peace and wasted time.
Both the patient self-assessed and professional POS versions are valid and with an acceptable internal consistency. POS detected significant clinical improvements during palliative care, at a time when patients are usually expected to deteriorate. These results suggest that there is room for substantial improvement in the management of patients with advanced disease, across all key domains-symptoms, psychological, information, social and spiritual.
评估结果的需求日益增加,但针对晚期疾病的评估指标却很少经过验证。我们旨在测试姑息治疗结果量表(POS)的有效性、可靠性和反应性,并分析向姑息治疗过渡后变化的预测因素。
第一阶段:多中心混合方法研究,包括对患者和工作人员进行认知和定性访谈、文化提炼和调整。第二阶段:连续收治入8家住院临终关怀机构和7个居家团队的癌症患者被要求完成POS、欧洲癌症研究与治疗组织核心问卷C15-PAL(EORTC QLQ-C15-PAL)和功能性癌症治疗-灵性健康量表(FACIT-Sp)(T0),以评估内部一致性、收敛效度和区分效度。6天后(T1),患者和工作人员完成POS,以评估对变化的反应性(T1-T0),以及患者自我评估的POS与工作人员完成的POS之间的一致性。最后,我们要求临终关怀机构在T1后24 - 48小时进行评估,以评估其可靠性(重测分析)。
第一阶段:评估了209份完整的POS问卷和29次认知访谈,进行了修订并替换了一个项目。第二阶段:接触了连续收治入15个姑息治疗团队的295名患者,175名(59.3%)符合条件,150名(85.7%)同意参与。40%的患者因病情严重而限制了同意参与的比例。我们发现了良好的收敛效度,POS、QLQ-C15-PAL和FACIT-Sp中相似项目之间存在强和中度相关性(r范围为0.5 - 0.8)。如假设的那样,QLQ-C15-PAL中的身体功能子量表与任何POS项目均无相关性(r范围为 - 0.16 - 0.02)。我们发现6个项目的两个版本的重测信度均可接受至良好。在评估的10个项目中的7个——疼痛、其他症状、患者和家属焦虑、信息、平静感和浪费时间方面,我们发现在姑息治疗的第一周有显著的临床改善。
患者自我评估版和专业版POS均有效且具有可接受的内部一致性。POS在姑息治疗期间检测到显著的临床改善,而此时通常预计患者病情会恶化。这些结果表明,在晚期疾病患者的管理方面,在所有关键领域——症状、心理、信息、社会和精神方面,仍有很大的改进空间。