Fatti Geoffrey, Shaikh Najma, Eley Brian, Grimwood Ashraf
a Kheth'Impilo , Cape Town , South Africa.
b Department of Paediatrics and Child Health , Red Cross War Memorial Children's Hospital, University of Cape Town , Cape Town , South Africa.
AIDS Care. 2016;28 Suppl 1(sup1):114-8. doi: 10.1080/09540121.2016.1148112. Epub 2016 Feb 28.
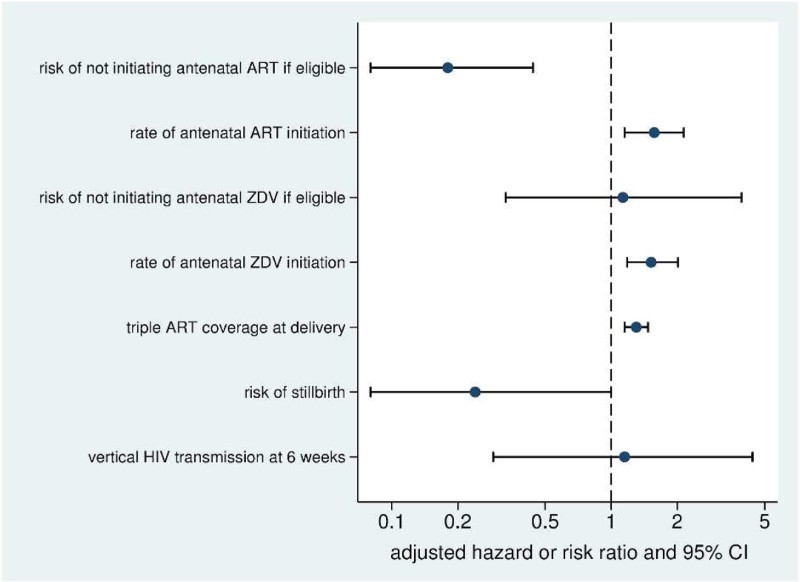
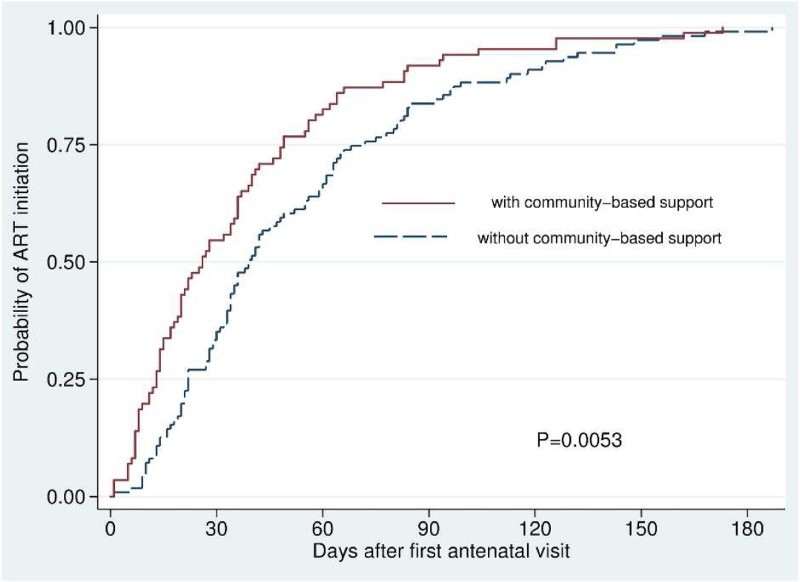
Antiretroviral treatment (ART) initiation in HIV-infected pregnant women in sub-Saharan Africa (SSA) remains inadequate, and there is a severe shortage of professional healthcare workers in the region. The effectiveness of community support programmes for HIV-infected pregnant women and their infants in SSA is unclear. This study compared initiation of maternal antiretrovirals and infant outcomes amongst HIV-infected pregnant women and their infants who received and did not receive community-based support (CBS) in a high HIV-prevalence setting in South Africa. A cohort study, including HIV-infected pregnant women and their infants, was conducted at three sentinel surveillance facilities between January 2009 and June 2012, utilising enhanced routine clinical data. Through home visits, CBS workers encouraged uptake of interventions in the ART cascade, provided HIV-related education, ART initiation counselling and psychosocial support. Outcomes were compared using Kaplan-Meier analyses and multivariable Cox and log-binomial regression. Amongst 1105 mother-infant pairs included, 264 (23.9%) received CBS. Amongst women eligible to start ART antenatally, women who received CBS had a reduced risk of not initiating antenatal ART, 5.4% vs. 30.3%; adjusted risk ratio (aRR) = 0.18 (95% CI: 0.08-0.44; P < .0001). Women who received CBS initiated antenatal ART with less delay after the first antenatal visit, median 26 days vs. 39 days; adjusted hazard ratio (aHR) = 1.57 (95% CI: 1.15-2.14; P = .004). Amongst women who initiated antenatal zidovudine (ZDV) to prevent vertical transmission, women who received CBS initiated ZDV with less delay, aHR = 1.52 (95% CI: 1.18-2.01; P = .001). Women who received CBS had a lower risk of stillbirth, 1.5% vs. 5.4%; aRR = 0.24 (95% CI: 0.07-1.00; P = .050). Pregnant women living with HIV who received CBS had improved antenatal triple ART initiation in eligible women, women initiated ART and ZDV with shorter delays, and had a lower risk of stillbirth. CBS is an intervention that shows promise in improving maternal and infant health in high HIV-prevalence settings.
在撒哈拉以南非洲地区(SSA),感染艾滋病毒的孕妇开始接受抗逆转录病毒治疗(ART)的情况仍然不理想,而且该地区专业医护人员严重短缺。SSA地区针对感染艾滋病毒的孕妇及其婴儿的社区支持项目的效果尚不清楚。本研究比较了在南非艾滋病毒高流行地区接受和未接受社区支持(CBS)的感染艾滋病毒的孕妇及其婴儿中孕产妇抗逆转录病毒药物的启动情况和婴儿结局。2009年1月至2012年6月期间,在三个哨点监测机构对包括感染艾滋病毒的孕妇及其婴儿在内的队列进行了研究,利用了强化的常规临床数据。通过家访,CBS工作人员鼓励在ART治疗流程中采用干预措施,提供与艾滋病毒相关的教育、ART启动咨询和心理社会支持。使用Kaplan-Meier分析以及多变量Cox和对数二项回归对结局进行比较。在纳入的1105对母婴中,264对(23.9%)接受了CBS。在符合产前开始ART条件的女性中,接受CBS的女性未开始产前ART的风险降低,分别为5.4%和30.3%;调整风险比(aRR)=0.18(95%CI:0.08 - 0.44;P <.0001)。接受CBS的女性在首次产前检查后开始产前ART的延迟时间更短,中位数为26天对39天;调整风险比(aHR)=1.57(95%CI:1.15 - 2.14;P = 0.004)。在开始产前使用齐多夫定(ZDV)以预防垂直传播的女性中,接受CBS的女性开始使用ZDV的延迟时间更短,aHR = 1.52(95%CI:1.18 - 2.01;P = 0.001)。接受CBS的女性死产风险较低,分别为1.5%和5.4%;aRR = 0.24(95%CI:0.07 - 1.00;P = 0.050)。接受CBS的感染艾滋病毒的孕妇在符合条件的女性中改善了产前三联ART的启动情况,女性开始ART和ZDV的延迟时间更短,且死产风险较低。CBS是一种在艾滋病毒高流行地区改善母婴健康方面显示出前景的干预措施。