Liu Wei, Wang Kun, Bao Quan, Sun Yi, Xing Bao-Cai
Hepatopancreatobiliary Surgery Department I, Key Laboratory of Carcinogenesis and Translational Research, Ministry of Education, Peking University School of Oncology, Beijing Cancer Hospital and Institute, No. 52, Fu-Cheng-Lu Street, Beijing, 100142, People's Republic of China.
World J Surg Oncol. 2016 Mar 2;14:62. doi: 10.1186/s12957-016-0811-y.
Hepatic resection has the highest local controllability that results in long-term survival for hepatocellular carcinoma (HCC). This study aimed to investigate the role of hepatic resection in selected patients of intermediate and advanced stage.
Clinical, pathological, and outcome data of 542 consecutive patients were retrospectively analyzed from a single center. The Kaplan-Meier method was used to estimate survival. Postoperative prognostic factors were evaluated using univariate and multivariate analyses.
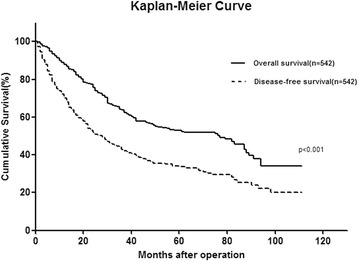
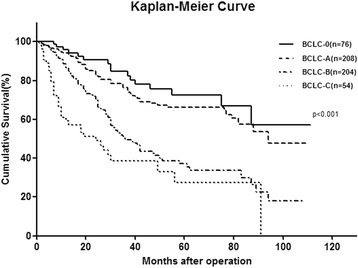
The 1-, 3-, and 5-year overall survival rates were 89.0, 64.3, and 53.0%, respectively. The 1-, 3-, and 5-year disease-free survival rates were 72.2, 44.5, and 34.2%, respectively. Preoperative α-fetoprotein level >400 ng/mL, macroscopic vascular invasion, microscopic portal vein thrombosis, multiple tumor nodules, and the largest tumor size >5 cm were significantly correlated with overall survival. When these clinical risk factors were used in a postoperative staging system, assigning one point for each factor, the total score was precisely predictive of long-term survival. For patients with surgery plus adjuvant TACE (transarterial chemoembolization), the median overall survival was 56 months (range 1-110 months) and the 5-year OS rate was 48.5%.
Hepatic resection is efficient and safe for HCC patients of intermediate and advanced stage. The adjuvant TACE should be recommended for HCC patients with poor risk factors.
肝切除术对肝细胞癌(HCC)具有最高的局部可控性,可实现长期生存。本研究旨在探讨肝切除术在中晚期特定患者中的作用。
回顾性分析来自单一中心的542例连续患者的临床、病理和结局数据。采用Kaplan-Meier法估计生存率。使用单因素和多因素分析评估术后预后因素。
1年、3年和5年总生存率分别为89.0%、64.3%和53.0%。1年、3年和5年无病生存率分别为72.2%、44.5%和34.2%。术前甲胎蛋白水平>400 ng/mL、肉眼可见血管侵犯、镜下门静脉血栓形成、多个肿瘤结节以及最大肿瘤直径>5 cm与总生存显著相关。当将这些临床危险因素用于术后分期系统,每个因素计1分时,总分可准确预测长期生存。对于接受手术加辅助经动脉化疗栓塞(TACE)的患者,中位总生存为56个月(范围1 - 110个月),5年总生存率为48.5%。
肝切除术对中晚期HCC患者有效且安全。对于具有不良危险因素的HCC患者,应推荐辅助TACE治疗。