Thompson J D, Chakraborty D P, Szczepura K, Tootell A K, Vamvakas I, Manning D J, Hogg P
Directorate of Radiography, University of Salford, Frederick Road Campus, Salford, Greater Manchester M6 6PU, United Kingdom and Department of Radiology, Furness General Hospital, University Hospitals of Morecambe Bay NHS Foundation Trust, Dalton Lane, Barrow-in-Furness LA14 4LF, United Kingdom.
Department of Radiology, University of Pittsburgh, FARP Building, Room 212, 3362 Fifth Avenue, Pittsburgh, Pennsylvania 15213.
Med Phys. 2016 Mar;43(3):1265-74. doi: 10.1118/1.4941017.
To evaluate nodule detection in an anthropomorphic chest phantom in computed tomography (CT) images reconstructed with adaptive iterative dose reduction 3D (AIDR(3D)) and filtered back projection (FBP) over a range of tube current-time product (mAs).
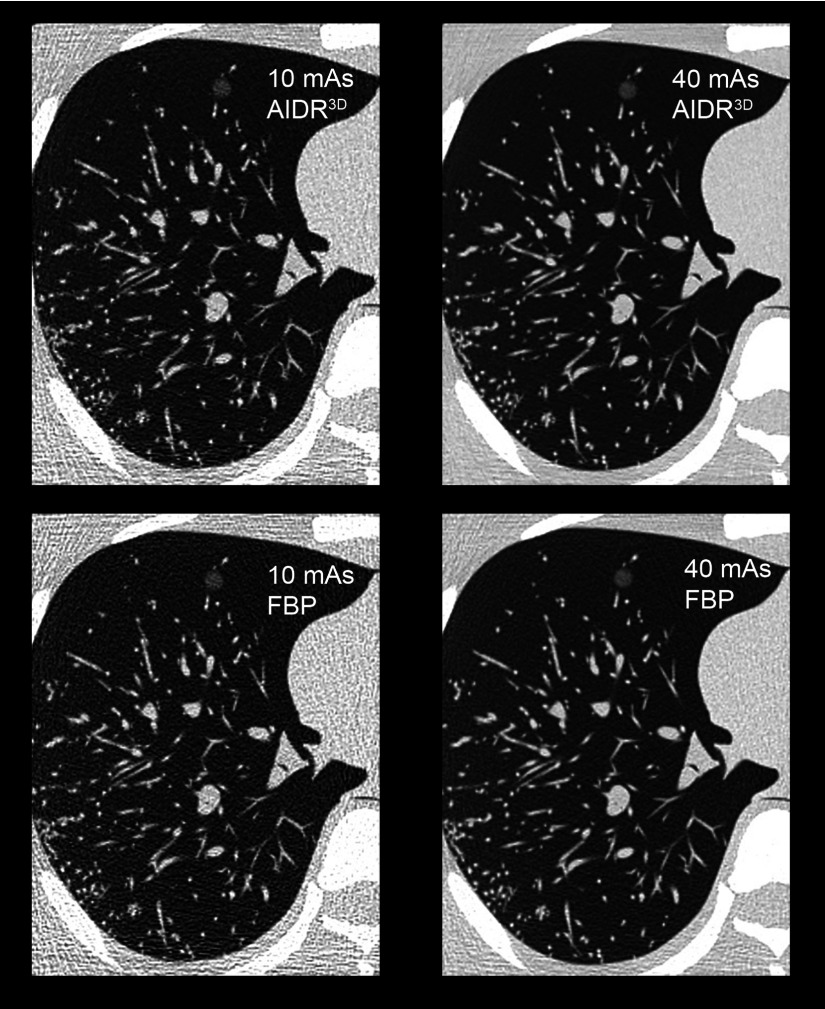
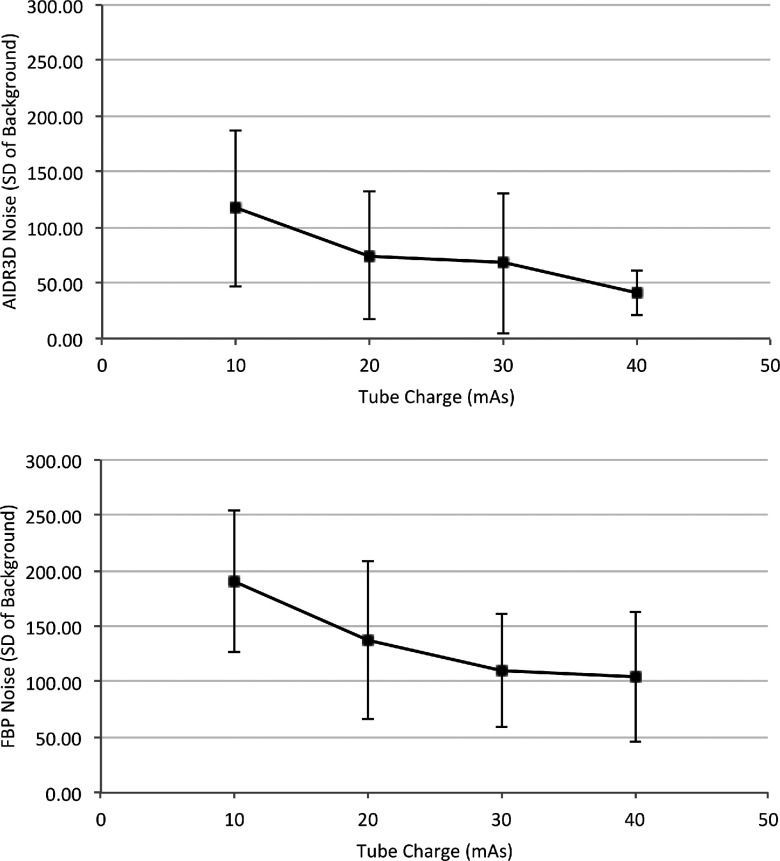
Two phantoms were used in this study: (i) an anthropomorphic chest phantom was loaded with spherical simulated nodules of 5, 8, 10, and 12 mm in diameter and +100, -630, and -800 Hounsfield units electron density; this would generate CT images for the observer study; (ii) a whole-body dosimetry verification phantom was used to ultimately estimate effective dose and risk according to the model of the BEIR VII committee. Both phantoms were scanned over a mAs range (10, 20, 30, and 40), while all other acquisition parameters remained constant. Images were reconstructed with both AIDR(3D) and FBP. For the observer study, 34 normal cases (no nodules) and 34 abnormal cases (containing 1-3 nodules, mean 1.35 ± 0.54) were chosen. Eleven observers evaluated images from all mAs and reconstruction methods under the free-response paradigm. A crossed-modality jackknife alternative free-response operating characteristic (JAFROC) analysis method was developed for data analysis, averaging data over the two factors influencing nodule detection in this study: mAs and image reconstruction (AIDR(3D) or FBP). A Bonferroni correction was applied and the threshold for declaring significance was set at 0.025 to maintain the overall probability of Type I error at α = 0.05. Contrast-to-noise (CNR) was also measured for all nodules and evaluated by a linear least squares analysis.
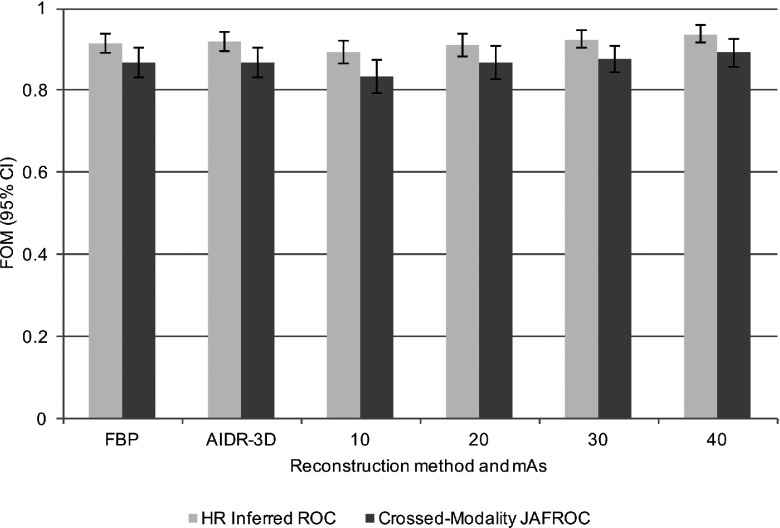
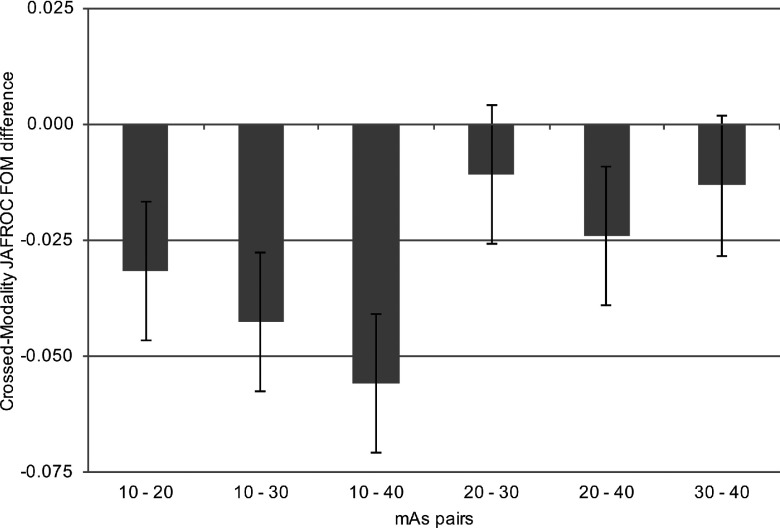
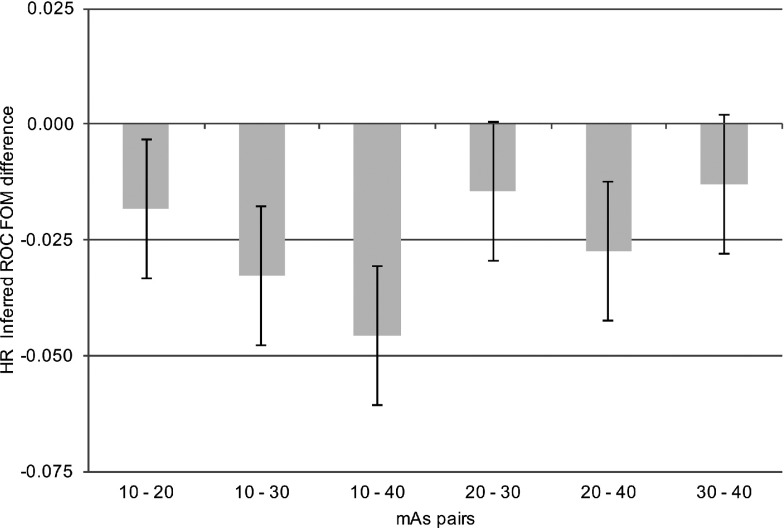
For random-reader fixed-case crossed-modality JAFROC analysis, there was no significant difference in nodule detection between AIDR(3D) and FBP when data were averaged over mAs [F(1, 10) = 0.08, p = 0.789]. However, when data were averaged over reconstruction methods, a significant difference was seen between multiple pairs of mAs settings [F(3, 30) = 15.96, p < 0.001]. Measurements of effective dose and effective risk showed the expected linear dependence on mAs. Nodule CNR was statistically higher for simulated nodules on images reconstructed with AIDR(3D) (p < 0.001).
No significant difference in nodule detection performance was demonstrated between images reconstructed with FBP and AIDR(3D). mAs was found to influence nodule detection, though further work is required for dose optimization.
评估在一系列管电流-时间乘积(毫安秒)条件下,采用自适应迭代剂量降低3D(AIDR(3D))和滤波反投影(FBP)重建的计算机断层扫描(CT)图像中,拟人化胸部体模内结节的检测情况。
本研究使用了两种体模:(i)一个拟人化胸部体模,其中加载了直径为5、8、10和12毫米且电子密度为+100、-630和-800亨氏单位的球形模拟结节;这将生成用于观察者研究的CT图像;(ii)一个全身剂量学验证体模,用于根据BEIR VII委员会的模型最终估计有效剂量和风险。两个体模均在毫安秒范围(10、20、30和40)内进行扫描,而所有其他采集参数保持不变。图像采用AIDR(3D)和FBP两种方法重建。对于观察者研究,选择了34例正常病例(无结节)和34例异常病例(包含1 - 3个结节,平均1.35 ± 0.54)。11名观察者在自由反应范式下评估所有毫安秒和重建方法的图像。开发了一种交叉模态留一法替代自由反应操作特征(JAFROC)分析方法用于数据分析,对本研究中影响结节检测的两个因素(毫安秒和图像重建(AIDR(3D)或FBP))的数据进行平均。应用了Bonferroni校正,将显著性声明阈值设定为0.025,以将I型错误的总体概率维持在α = 0.05。还测量了所有结节的对比度噪声比(CNR),并通过线性最小二乘法分析进行评估。
对于随机读者固定病例交叉模态JAFROC分析,当数据在毫安秒上进行平均时,AIDR(3D)和FBP在结节检测方面无显著差异[F(1, 10) = 0.08,p = 0.789]。然而,当数据在重建方法上进行平均时,多对毫安秒设置之间存在显著差异[F(3, 30) = 15.96,p < 0.001]。有效剂量和有效风险的测量显示出对毫安秒的预期线性依赖性。对于用AIDR(3D)重建的图像上的模拟结节,结节CNR在统计学上更高(p < 0.001)。
FBP和AIDR(3D)重建的图像在结节检测性能上未显示出显著差异。发现毫安秒会影响结节检测,不过剂量优化还需要进一步的研究工作。