Rasmussen Kirsten C, Højskov Michael, Johansson Pär I, Kridina Irina, Kistorp Thomas, Salling Lisbeth, Nielsen Henning B, Ruhnau Birgitte, Pedersen Tom, Secher Niels H
From the Department of Anesthesiology (KCR, MH, IK, TK, HBN, BR, NHS); Department of Urology (LS); Center of Head and Orthopaedic Surgery (TP); Rigshospitalet, University of Copenhagen; Department of Transfusion Medicine, Rigshospitalet and Department of Surgery, Denmark, and University of Texas Health Medical School, Houston, TX, USA (PIJ).
Medicine (Baltimore). 2016 Mar;95(9):e2720. doi: 10.1097/MD.0000000000002720.
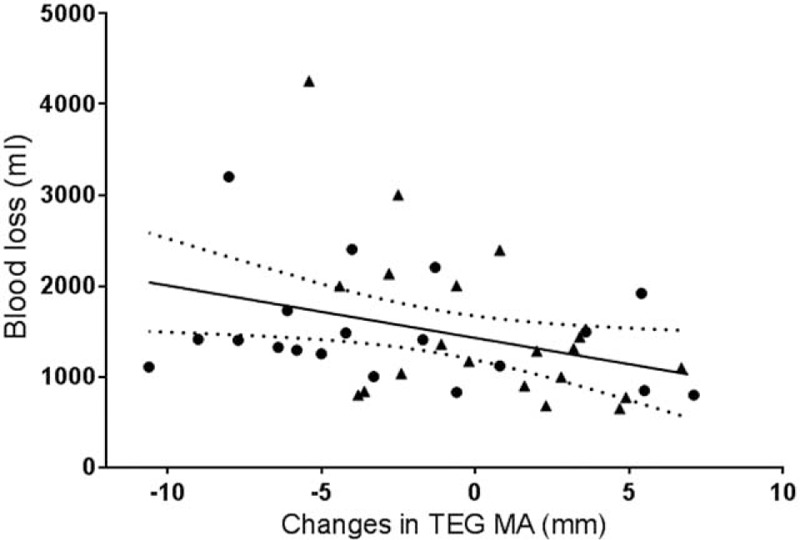
For patients exposed to a massive blood loss during surgery, maintained coagulation competence is important. It is less obvious whether coagulation competence influences bleeding during elective surgery where patients are exposed to infusion of a crystalloid or a colloid. This randomized controlled trial evaluates whether administration of 5% human albumin (HA) or lactated Ringer solution (LR) affects coagulation competence and in turn blood loss during cystectomy due to bladder cancer. Forty patients undergoing radical cystectomy were included to receive either 5% HA (n = 20) or LR (n = 20). Nineteen patients were analyzed in the HA group and 20 patients in the lactated Ringer group. Blinded determination of the blood loss was similar in the 2 groups of patients: 1658 (800-3300) mL with the use of HA and 1472 (700-4330) mL in the lactated Ringer group (P = 0.45). Yet, by thrombelastography (TEG) evaluated coagulation competence, albumin affected clot growth (TEG-angle 69 ± 5 vs 74° ± 3°, P < 0.01) and strength (TEG-MA: 59 ± 6 vs 67 ± 6 mm, P < 0.001) more than LR. Furthermore, by multivariate linear regression analyses reduced TEG-MA was independently associated with the blood loss (P = 0.042) while administration of albumin was related to the changes in TEG-MA (P = 0.029), aPPT (P < 0.022), and INR (P < 0.033). This randomized controlled trial demonstrates that administration of HA does not affect the blood loss as compared to infusion of LR. Also the use of HA did not affect the need for blood transfusion, the incidence of postoperative complications, or the hospital in-stay. Yet, albumin decreases coagulation competence during major surgery and the blood loss is related to TEG-MA rather than to plasma coagulation variables.
对于在手术中面临大量失血的患者,维持凝血功能很重要。而在择期手术中,当患者接受晶体液或胶体液输注时,凝血功能是否会影响出血情况则不太明确。这项随机对照试验评估了输注5%人血白蛋白(HA)或乳酸林格氏液(LR)是否会影响凝血功能,进而影响因膀胱癌行膀胱切除术时的失血量。40例行根治性膀胱切除术的患者被纳入研究,分别接受5% HA(n = 20)或LR(n = 20)。HA组分析了19例患者,乳酸林格氏液组分析了20例患者。两组患者失血量的盲法测定结果相似:使用HA组为1658(800 - 3300)mL,乳酸林格氏液组为1472(700 - 4330)mL(P = 0.45)。然而,通过血栓弹力图(TEG)评估凝血功能发现,白蛋白对血凝块生长(TEG角度:69±5° vs 74°±3°,P < 0.01)和强度(TEG - MA:59±6 vs 67±6 mm,P < 0.001)的影响比LR更大。此外,通过多变量线性回归分析,降低的TEG - MA与失血量独立相关(P = 0.042),而白蛋白的输注与TEG - MA的变化(P = 0.029)、活化部分凝血活酶时间(aPPT,P < 0.022)和国际标准化比值(INR,P < 0.033)相关。这项随机对照试验表明,与输注LR相比,输注HA不会影响失血量。使用HA也不影响输血需求、术后并发症发生率或住院时间。然而,白蛋白会降低大手术期间的凝血功能,且失血量与TEG - MA相关,而非与血浆凝血变量相关。