Peters Inge T A, Hilders Carina G J M, Sier Cornelis F M, Vahrmeijer Alexander L, Smit Vincent T H B M, Baptist Trimbos J, Kuppen Peter J K
Department of Gynecology, Leiden University Medical Center, Leiden, The Netherlands.
Department of Gynecology, Reinier de Graaf Hospital, Delft, The Netherlands.
Arch Gynecol Obstet. 2016 Aug;294(2):385-93. doi: 10.1007/s00404-016-4036-7. Epub 2016 Mar 5.
The safety of ovarian tissue autotransplantation in oncology patients cannot be ensured, as current tumor-detection methods compromise the ovarian tissue viability. Although non-destructive methods (for instance near-infrared fluorescence imaging) can discriminate malignant from healthy tissues while leaving the examined tissues unaffected, they require specific cell-surface tumor markers. We determined which tumor markers are suitable targets for tumor-specific imaging to exclude the presence of breast cancer cells in ovarian tissue.
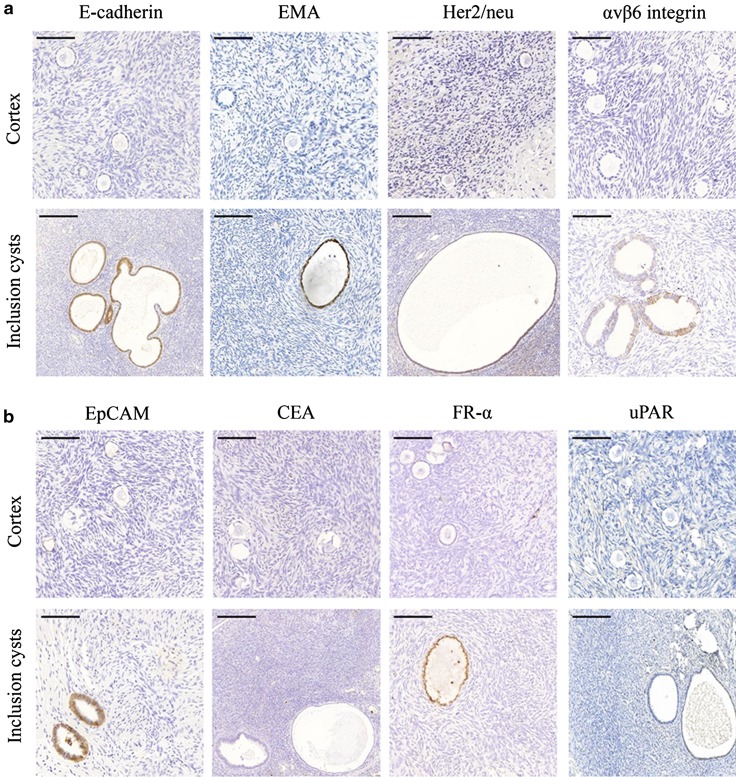
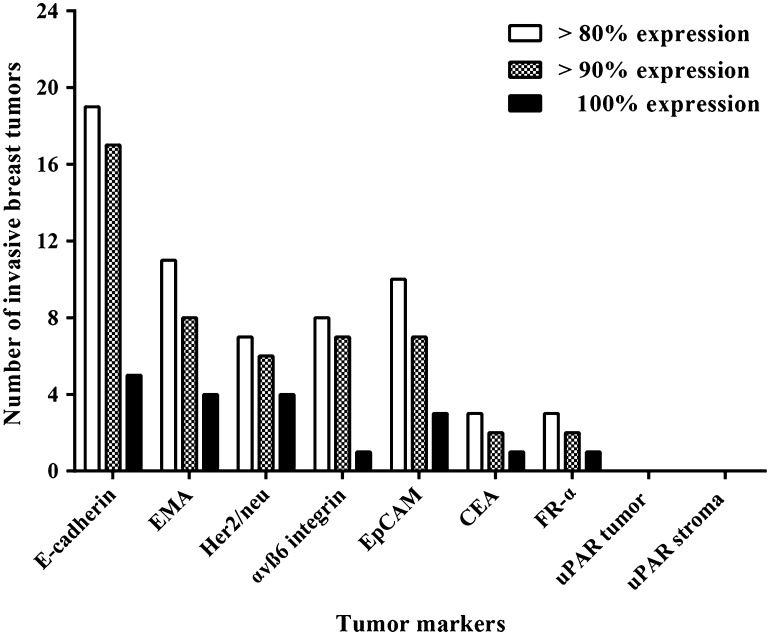
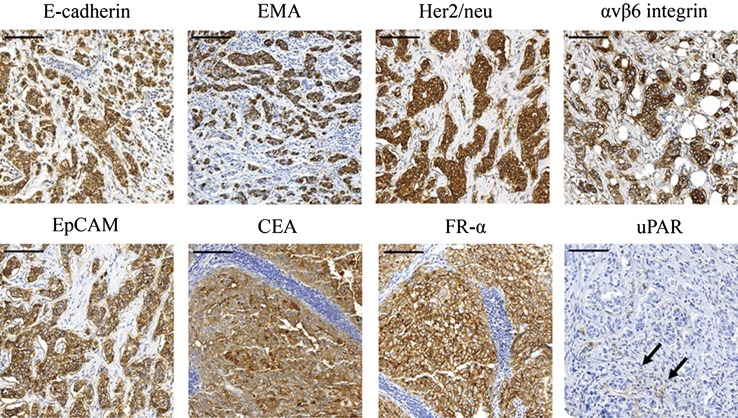
Immunohistochemistry was performed on formalin-fixed, paraffin-embedded specimens of ten ovaries from premenopausal patients. Additionally, we screened a tissue microarray containing tumor tissue cores from 24 breast cancer patients being eligible for ovarian tissue cryopreservation. The following cell-surface tumor markers were tested: E-cadherin, EMA (epithelial membrane antigen), Her2/neu (human epidermal growth factor receptor type 2), αvβ6 integrin, EpCAM (epithelial cell adhesion molecule), CEA (carcinoembryonic antigen), FR-α (folate receptor-alpha), and uPAR (urokinase-type plasminogen activator receptor). For each tumor, the percentage of positive breast tumor cells was measured.
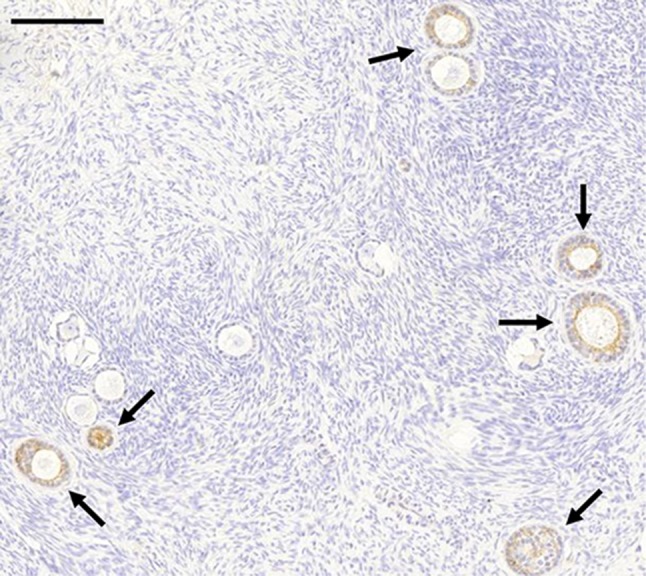
None of the ten ovaries were positive for any of the markers tested. However, all markers (except CEA and uPAR) were present on epithelial cells of inclusion cysts. E-cadherin was present in the majority of breast tumors: ≥90 % of tumor cells were positive for E-cadherin in 17 out of 24 tumors, and 100 % of tumor cells were positive in 5 out of 24 tumors.
Of the markers tested, E-cadherin is the most suitable marker for a tumor-specific probe in ovarian tissue. Methods are required to distinguish inclusion cysts from breast tumor cells.
肿瘤患者卵巢组织自体移植的安全性无法得到保证,因为目前的肿瘤检测方法会损害卵巢组织的活力。尽管非破坏性方法(如近红外荧光成像)能够在不影响被检查组织的情况下区分恶性组织和健康组织,但它们需要特定的细胞表面肿瘤标志物。我们确定了哪些肿瘤标志物是肿瘤特异性成像的合适靶点,以排除卵巢组织中乳腺癌细胞的存在。
对来自绝经前患者的10个卵巢的福尔马林固定、石蜡包埋标本进行免疫组织化学检测。此外,我们筛选了一个组织芯片,其中包含24例符合卵巢组织冷冻保存条件的乳腺癌患者的肿瘤组织芯。检测了以下细胞表面肿瘤标志物:E-钙黏蛋白、上皮膜抗原(EMA)、人表皮生长因子受体2(Her2/neu)、αvβ6整合素、上皮细胞黏附分子(EpCAM)、癌胚抗原(CEA)、叶酸受体α(FR-α)和尿激酶型纤溶酶原激活剂受体(uPAR)。对于每个肿瘤,测量阳性乳腺肿瘤细胞的百分比。
所检测的10个卵巢中,没有一个对任何检测的标志物呈阳性。然而,所有标志物(CEA和uPAR除外)均存在于包涵囊肿的上皮细胞中。E-钙黏蛋白存在于大多数乳腺肿瘤中:24个肿瘤中有17个肿瘤中≥90%的肿瘤细胞E-钙黏蛋白呈阳性,24个肿瘤中有5个肿瘤中100%的肿瘤细胞呈阳性。
在所检测的标志物中,E-钙黏蛋白是卵巢组织中肿瘤特异性探针最适合的标志物。需要有方法来区分包涵囊肿和乳腺肿瘤细胞。