Wirth Rainer, Dziewas Rainer, Beck Anne Marie, Clavé Pere, Hamdy Shaheen, Heppner Hans Juergen, Langmore Susan, Leischker Andreas Herbert, Martino Rosemary, Pluschinski Petra, Rösler Alexander, Shaker Reza, Warnecke Tobias, Sieber Cornel Christian, Volkert Dorothee
Department for Internal Medicine and Geriatrics, St Marien-Hospital Borken, Borken, Germany; Institute for Biomedicine of Aging, Friedrich-Alexander-Universität Erlangen-Nürnberg, Nürnberg, Germany.
Department of Neurology, University Hospital Münster, Münster, Germany.
Clin Interv Aging. 2016 Feb 23;11:189-208. doi: 10.2147/CIA.S97481. eCollection 2016.
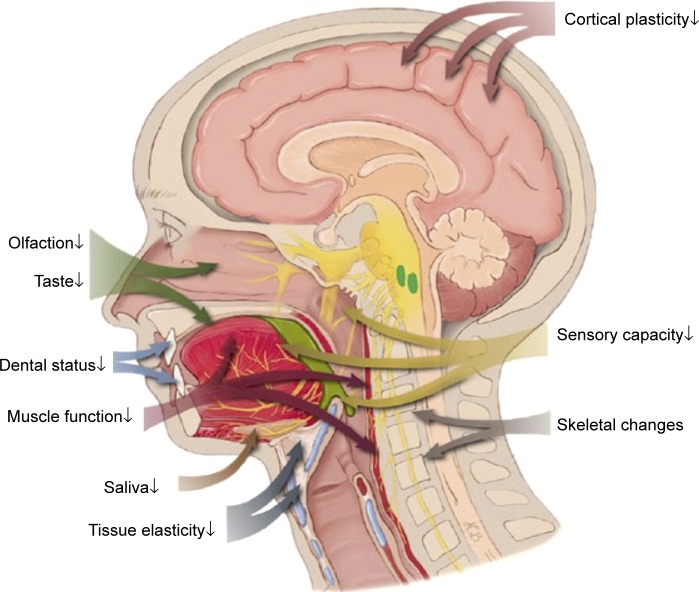
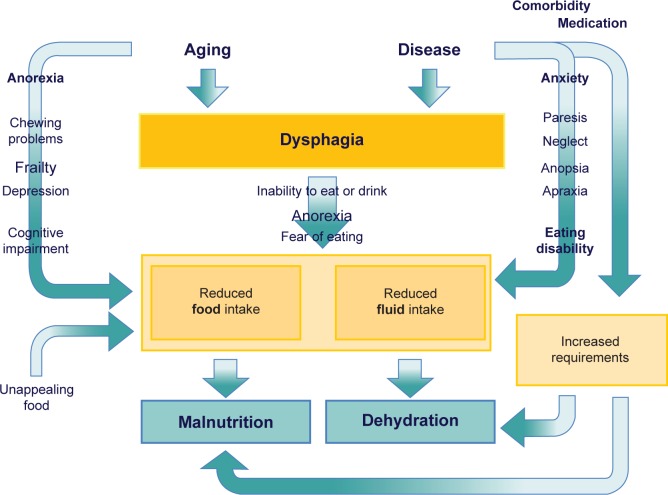
Oropharyngeal dysphagia (OD) is a highly prevalent and growing condition in the older population. Although OD may cause very severe complications, it is often not detected, explored, and treated. Older patients are frequently unaware of their swallowing dysfunction which is one of the reasons why the consequences of OD, ie, aspiration, dehydration, and malnutrition, are regularly not attributed to dysphagia. Older patients are particularly vulnerable to dysphagia because multiple age-related changes increase the risk of dysphagia. Physicians in charge of older patients should be aware that malnutrition, dehydration, and pneumonia are frequently caused by (unrecognized) dysphagia. The diagnosis is particularly difficult in the case of silent aspiration. In addition to numerous screening tools, videofluoroscopy was the traditional gold standard of diagnosing OD. Recently, the fiberoptic endoscopic evaluation of swallowing is increasingly utilized because it has several advantages. Besides making a diagnosis, fiberoptic endoscopic evaluation of swallowing is applied to evaluate the effectiveness of therapeutic maneuvers and texture modification of food and liquids. In addition to swallowing training and nutritional interventions, newer rehabilitation approaches of stimulation techniques are showing promise and may significantly impact future treatment strategies.
口咽吞咽困难(OD)在老年人群中是一种高度普遍且日益常见的病症。尽管OD可能会引发非常严重的并发症,但它常常未被检测、探究和治疗。老年患者往往未意识到自己的吞咽功能障碍,这也是OD的后果(即误吸、脱水和营养不良)常常未被归因于吞咽困难的原因之一。老年患者特别容易出现吞咽困难,因为多种与年龄相关的变化会增加吞咽困难的风险。负责老年患者的医生应意识到,营养不良、脱水和肺炎常常是由(未被识别的)吞咽困难引起的。在隐性误吸的情况下,诊断尤为困难。除了众多筛查工具外,视频荧光吞咽造影检查曾是诊断OD的传统金标准。近来,纤维内镜吞咽功能检查越来越多地被使用,因为它有几个优点。除了进行诊断外,纤维内镜吞咽功能检查还用于评估治疗措施的效果以及食物和液体质地的调整。除了吞咽训练和营养干预外应用外,刺激技术等新的康复方法显示出前景,可能会对未来的治疗策略产生重大影响。