Dewland Thomas A, Bibbins-Domingo Kirsten, Lin Feng, Vittinghoff Eric, Foster Elyse, Ogunyankin Kofo O, Lima Joao A, Jacobs David R, Hu Donglei, Burchard Esteban G, Marcus Gregory M
Electrophysiology Section, Division of Cardiology, Department of Medicine, University of California San Francisco, San Francisco, California, United States of America.
Knight Cardiovascular Institute, Oregon Health & Science University, Portland, Oregon, United States of America.
PLoS One. 2016 Mar 17;11(3):e0151559. doi: 10.1371/journal.pone.0151559. eCollection 2016.
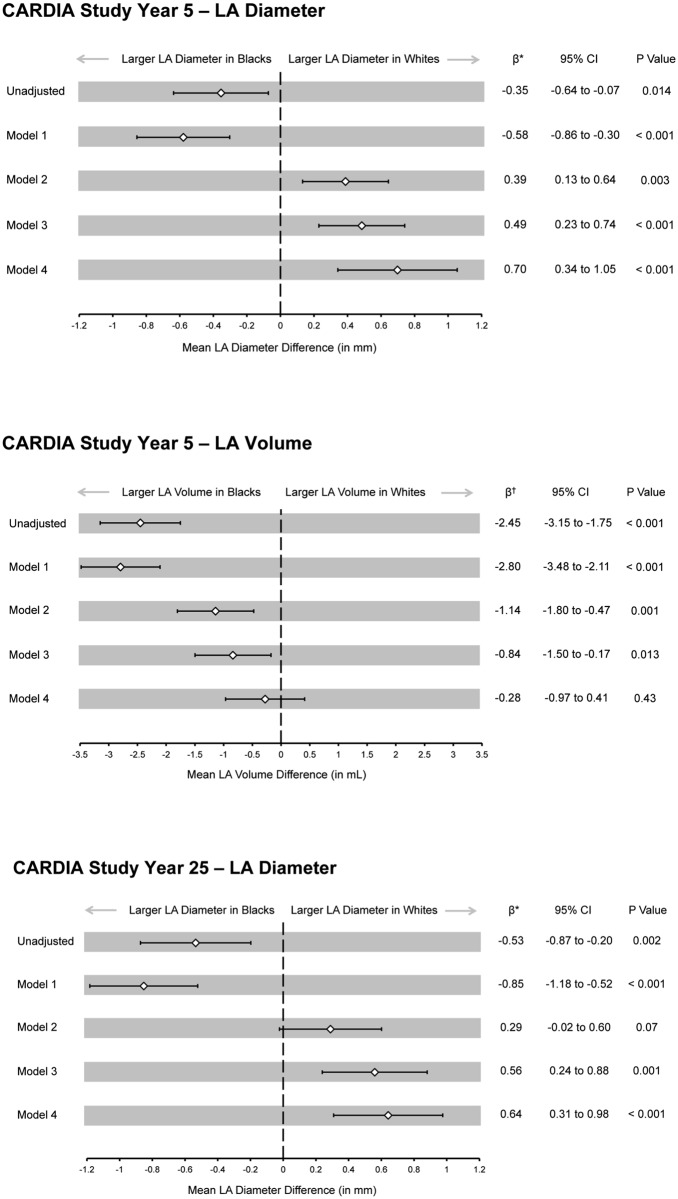
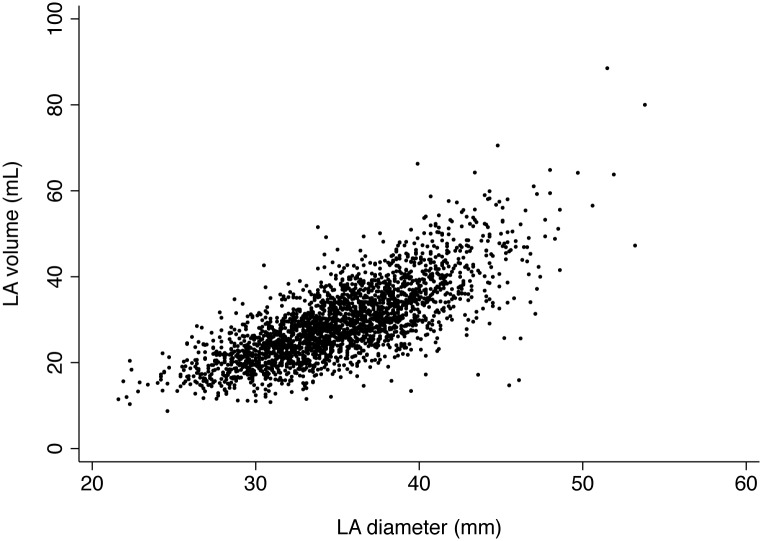
Whites have an increased risk of atrial fibrillation (AF) compared to Blacks. The mechanism underlying this association is unknown. Left atrial (LA) size is an important AF risk factor, and studies in older adults suggest Whites have larger LA diameters. However, because AF itself causes LA dilation, LA size differences may be due to greater subclinical AF among older Whites. We therefore assessed for racial differences in LA size among young adults at low AF risk. The Coronary Artery Risk Development in Young Adults (CARDIA) study enrolled White and Black participants between 18 and 30 years of age. LA diameter was measured in a subset of participants using echocardiography at Year 5 (n = 4,201) and Year 25 (n = 3,373) of follow up. LA volume was also assessed at Year 5 (n = 2,489). Multivariate linear regression models were used to determine the adjusted association between race and LA size. In unadjusted analyses, mean LA diameter was significantly larger among Blacks compared to Whites both at Year 5 (35.5 ± 4.8 mm versus 35.1 ± 4.5 mm, p = 0.01) and Year 25 (37.4 ± 5.1 mm versus 36.8 ± 4.9 mm, p = 0.002). After adjusting for demographics, comorbidities, and echocardiographic parameters, Whites demonstrated an increased LA diameter (0.7 mm larger at Year 5, 95% CI 0.3-1.1, p<0.001; 0.6 mm larger at Year 25, 95% CI 0.3-1.0, p<0.001). There was no significant association between race and adjusted Year 5 LA volume. In conclusion, in a young, well-characterized cohort, the larger adjusted LA diameter among White participants suggests inherent differences in atrial structure may partially explain the higher risk of AF in Whites. The incongruent associations between race, LA diameter, and LA volume suggest that LA geometry, rather than size alone, may have implications for AF risk.
与黑人相比,白人患心房颤动(AF)的风险更高。这种关联背后的机制尚不清楚。左心房(LA)大小是一个重要的房颤风险因素,对老年人的研究表明白人的左心房直径更大。然而,由于房颤本身会导致左心房扩张,左心房大小差异可能是由于老年白人中存在更多的亚临床房颤。因此,我们评估了低房颤风险的年轻成年人中左心房大小的种族差异。青年冠状动脉风险发展(CARDIA)研究招募了年龄在18至30岁之间的白人和黑人参与者。在随访的第5年(n = 4,201)和第25年(n = 3,373),使用超声心动图测量了一部分参与者的左心房直径。在第5年(n = 2,489)也评估了左心房容积。使用多变量线性回归模型来确定种族与左心房大小之间的校正关联。在未校正的分析中,黑人的平均左心房直径在第5年(35.5±4.8毫米对35.1±4.5毫米,p = 0.01)和第25年(37.4±5.1毫米对36.8±4.9毫米,p = 0.002)均显著大于白人。在调整了人口统计学、合并症和超声心动图参数后,白人的左心房直径增加(第5年大0.7毫米,95%CI 0.3 - 1.1,p<0.001;第25年大0.6毫米,95%CI 0.3 - 1.0,p<0.001)。种族与校正后的第5年左心房容积之间无显著关联。总之,在一个年轻的、特征明确的队列中,白人参与者校正后的左心房直径较大表明心房结构的固有差异可能部分解释了白人患房颤风险较高的原因。种族、左心房直径和左心房容积之间不一致的关联表明,左心房几何形状而非单纯的大小可能对房颤风险有影响。