Bell Lucy C K, Pollara Gabriele, Pascoe Mellissa, Tomlinson Gillian S, Lehloenya Rannakoe J, Roe Jennifer, Meldau Richard, Miller Robert F, Ramsay Alan, Chain Benjamin M, Dheda Keertan, Noursadeghi Mahdad
Division of Infection and Immunity, University College London, London, United Kingdom.
Lung Infection and Immunity Unit, Division of Pulmonology and UCT Lung Institute, Department of Medicine, University of Cape Town, Cape Town, South Africa.
PLoS Pathog. 2016 Mar 17;12(3):e1005469. doi: 10.1371/journal.ppat.1005469. eCollection 2016 Mar.
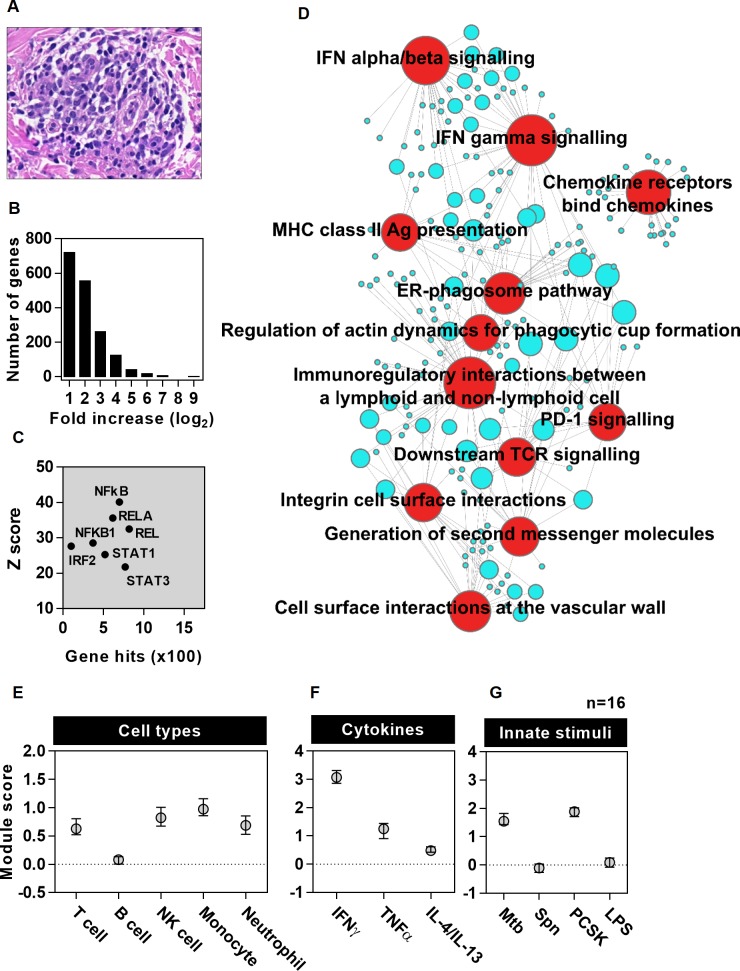
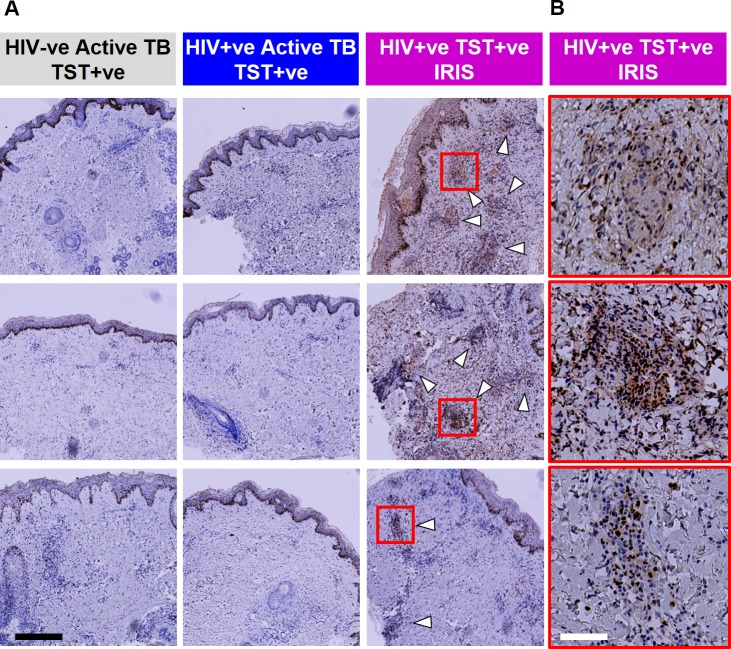
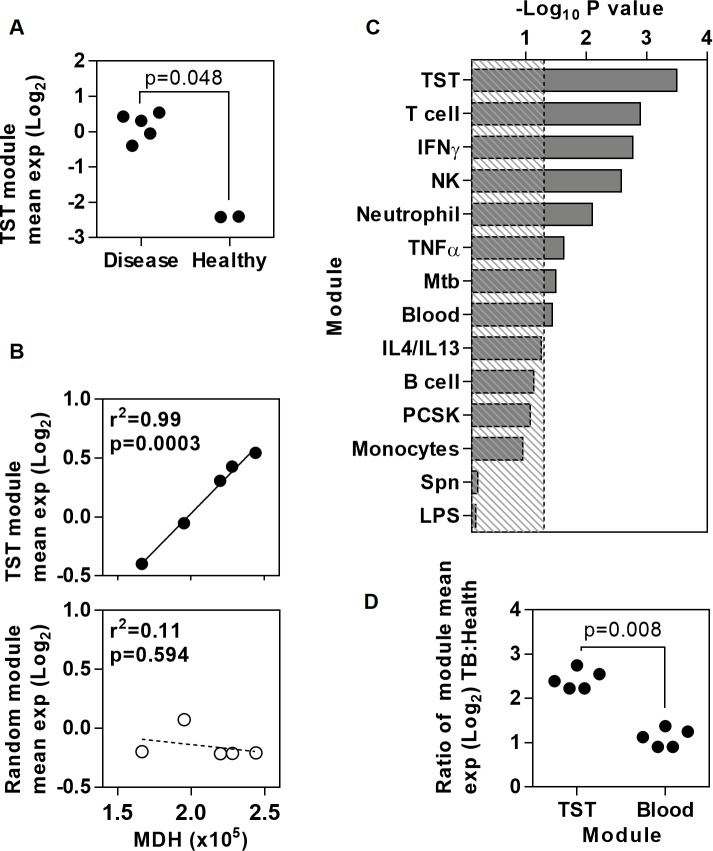
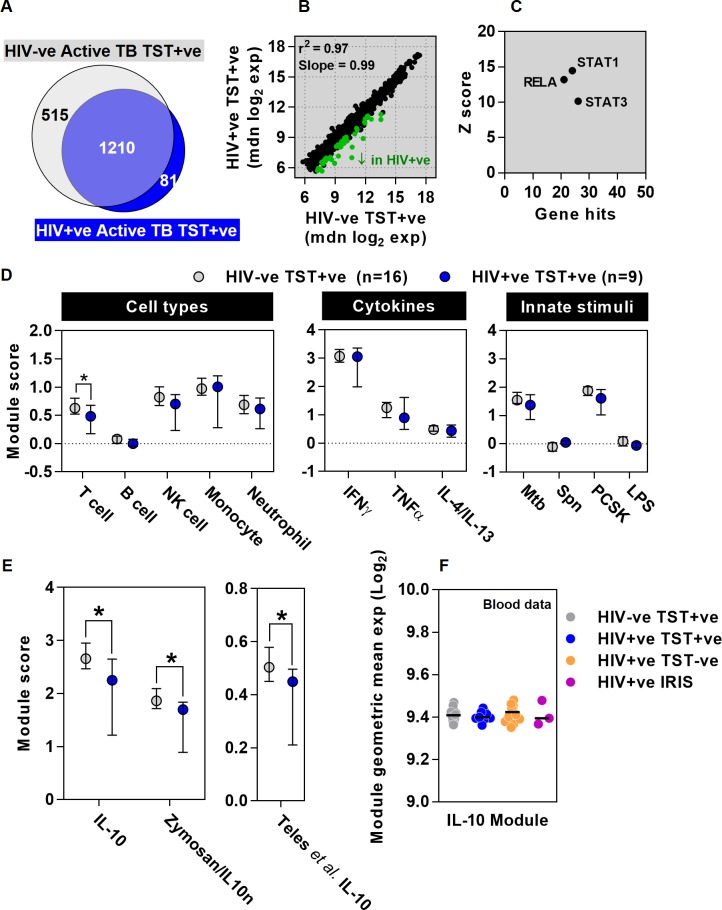
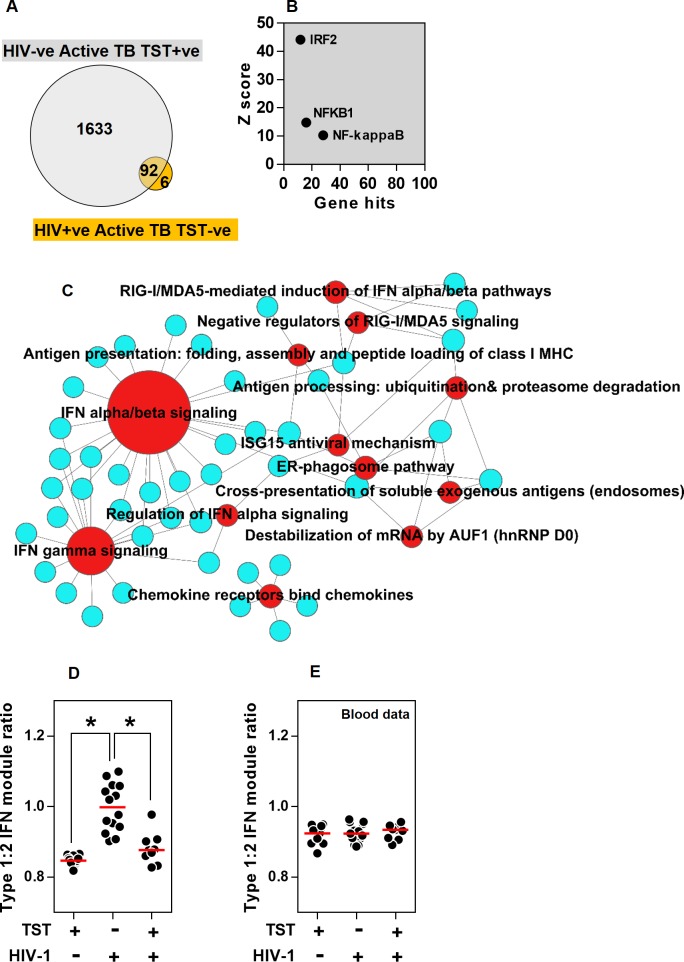
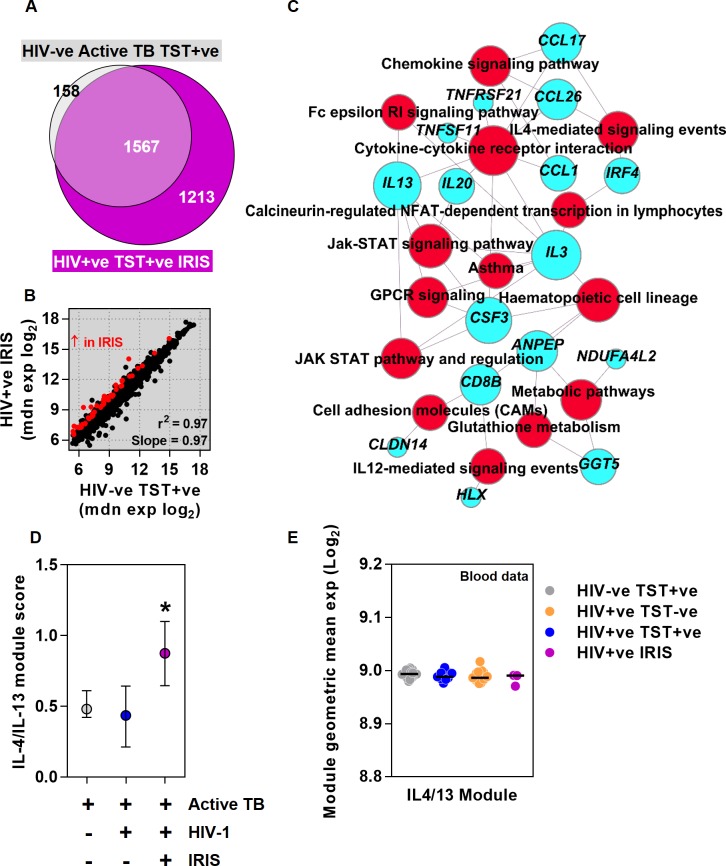
Increased risk of tuberculosis (TB) associated with HIV-1 infection is primarily attributed to deficient T helper (Th)1 immune responses, but most people with active TB have robust Th1 responses, indicating that these are not sufficient to protect against disease. Recent findings suggest that favourable outcomes following Mycobacterium tuberculosis infection arise from finely balanced inflammatory and regulatory pathways, achieving pathogen control without immunopathology. We hypothesised that HIV-1 and antiretroviral therapy (ART) exert widespread changes to cell mediated immunity, which may compromise the optimal host protective response to TB and provide novel insights into the correlates of immune protection and pathogenesis. We sought to define these effects in patients with active TB by transcriptional profiling of tuberculin skin tests (TST) to make comprehensive molecular level assessments of in vivo human immune responses at the site of a standardised mycobacterial challenge. We showed that the TST transcriptome accurately reflects the molecular pathology at the site of human pulmonary TB, and used this approach to investigate immune dysregulation in HIV-1/TB co-infected patients with distinct clinical phenotypes associated with TST reactivity or anergy and unmasking TB immune reconstitution inflammatory syndrome (IRIS) after initiation of ART. HIV-1 infected patients with positive TSTs exhibited preserved Th1 responses but deficient immunoregulatory IL10-inducible responses. Those with clinically negative TSTs revealed profound anergy of innate as well as adaptive immune responses, except for preservation of type 1 interferon activity, implicated in impaired anti-mycobacterial immunity. Patients with unmasking TB IRIS showed recovery of Th1 immunity to normal levels, but exaggerated Th2-associated responses specifically. These mechanisms of immune dysregulation were localised to the tissue microenvironment and not evident in peripheral blood. TST molecular profiling categorised different mechanisms of immunological dysfunction in HIV-1 infection beyond the effects on CD4 T cells, each associated with increased risk of TB disease and amenable to host-directed therapies.
与HIV-1感染相关的结核病(TB)风险增加主要归因于辅助性T(Th)1免疫反应不足,但大多数活动性结核病患者具有强大的Th1反应,这表明这些反应不足以预防疾病。最近的研究结果表明,结核分枝杆菌感染后的良好结局源于炎症和调节途径的精细平衡,在不产生免疫病理的情况下实现病原体控制。我们假设HIV-1和抗逆转录病毒疗法(ART)会对细胞介导的免疫产生广泛影响,这可能会损害宿主对结核病的最佳保护反应,并为免疫保护和发病机制的相关性提供新的见解。我们试图通过结核菌素皮肤试验(TST)的转录谱分析来确定活动性结核病患者的这些影响,以便在标准化分枝杆菌攻击部位对体内人类免疫反应进行全面的分子水平评估。我们表明,TST转录组准确反映了人类肺结核部位的分子病理学,并使用这种方法研究了HIV-1/TB合并感染患者的免疫失调,这些患者具有与TST反应性或无反应性相关的不同临床表型,并在开始ART后揭示了结核病免疫重建炎症综合征(IRIS)。TST呈阳性的HIV-1感染患者表现出保留的Th1反应,但免疫调节性IL10诱导反应不足。那些TST临床阴性的患者除了保留1型干扰素活性外,先天性和适应性免疫反应均表现出严重的无反应性,这与抗分枝杆菌免疫受损有关。出现结核病IRIS的患者Th1免疫恢复到正常水平,但Th2相关反应尤其过度。这些免疫失调机制局限于组织微环境,在外周血中不明显。TST分子谱分析对HIV-1感染中免疫功能障碍的不同机制进行了分类,这些机制超出了对CD4 T细胞的影响,每种机制都与结核病风险增加相关,并且适合宿主导向疗法。