Bobb Morgan R, Van Heukelom Paul G, Faine Brett A, Ahmed Azeemuddin, Messerly Jeffrey T, Bell Gregory, Harland Karisa K, Simon Christian, Mohr Nicholas M
Department of Emergency Medicine, University of Iowa Carver College of Medicine, Iowa City, IA.
Program in Bioethics and Humanities, Department of Internal Medicine, University of Iowa Carver College of Medicine, Iowa City, IA.
Acad Emerg Med. 2016 Jul;23(7):759-65. doi: 10.1111/acem.12966. Epub 2016 Jun 18.
Telemedicine networks are beginning to provide an avenue for conducting emergency medicine research, but using telemedicine to recruit participants for clinical trials has not been validated. The goal of this consent study was to determine whether patient comprehension of telemedicine-enabled research informed consent is noninferior to standard face-to-face (F2F) research informed consent.
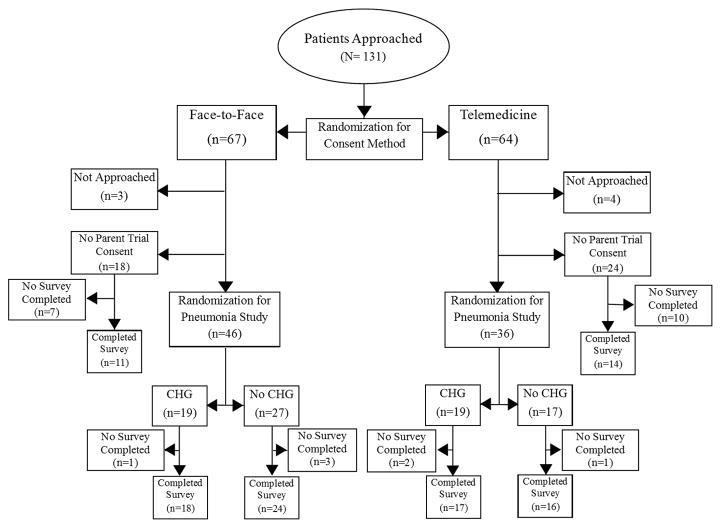
A prospective, open-label randomized controlled trial was performed in a 60,000-visit Midwestern academic emergency department (ED) to test whether telemedicine-enabled research informed consent provided noninferior comprehension compared with standard consent. This study was conducted as part of a parent clinical trial evaluating the effectiveness of 0.12% oral chlorhexidine gluconate in preventing hospital-acquired pneumonia among adult ED patients with expected hospital admission. Prior to being recruited into the study, potential participants were randomized in a 1:1 allocation ratio to consent by telemedicine versus standard F2F consent. Telemedicine connectivity was provided using a commercially available interface (REACH platform, Vidyo Inc.) to an emergency physician located in another part of the ED. Comprehension of research consent (primary outcome) was measured using the modified quality of informed consent (QuIC) instrument, a validated tool for measuring research informed consent comprehension. Parent trial accrual rate and qualitative survey data were secondary outcomes.
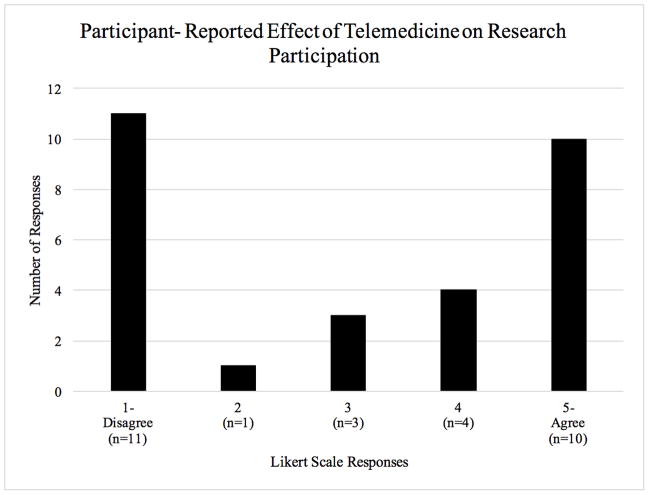
A total of 131 patients were randomized (n = 64, telemedicine), and 101 QuIC surveys were completed. Comprehension of research informed consent using telemedicine was not inferior to F2F consent (QuIC scores 74.4 ± 8.1 vs. 74.4 ± 6.9 on a 100-point scale, p = 0.999). Subjective understanding of consent (p = 0.194) and parent trial study accrual rates (56% vs. 69%, p = 0.142) were similar.
Telemedicine is noninferior to F2F consent for delivering research informed consent, with no detected differences in comprehension and patient-reported understanding. This consent study will inform design of future telemedicine-enabled clinical trials.
远程医疗网络开始为开展急诊医学研究提供了一条途径,但利用远程医疗招募临床试验参与者尚未得到验证。本知情同意研究的目的是确定患者对基于远程医疗的研究知情同意书的理解是否不劣于标准的面对面(F2F)研究知情同意书。
在一家年就诊量达60000人次的中西部学术性急诊科进行了一项前瞻性、开放标签随机对照试验,以测试基于远程医疗的研究知情同意书与标准同意书相比是否能提供不劣的理解度。本研究是一项母临床试验的一部分,该母临床试验评估0.12%葡萄糖酸氯己定口服溶液在预防预期住院的成年急诊科患者医院获得性肺炎方面的有效性。在被纳入研究之前,潜在参与者按1:1的分配比例随机分为通过远程医疗同意组和标准面对面同意组。使用商用接口(REACH平台,Vidyo公司)向位于急诊科另一区域的急诊医生提供远程医疗连接。使用改良的知情同意质量(QuIC)工具测量对研究同意书的理解(主要结局),该工具是一种用于测量研究知情同意理解度的经过验证的工具。母试验入组率和定性调查数据为次要结局。
共131例患者被随机分组(远程医疗组n = 64),完成了101份QuIC调查问卷。使用远程医疗对研究知情同意书的理解不劣于面对面同意(在100分制中,QuIC评分分别为74.4±8.1和74.4±6.9,p = 0.999)。对同意书的主观理解(p = 0.194)和母试验研究入组率(分别为56%和69%,p = 0.142)相似。
在提供研究知情同意书方面,远程医疗不劣于面对面同意,在理解度和患者报告的理解方面未发现差异。本知情同意研究将为未来基于远程医疗的临床试验设计提供参考。